In low-income countries, the cost of digestive endoscopy procedures is often unknown, yet its understanding is crucial for including them in the universal health coverage benefit package. The management of digestive endoscopy requires substantial financial contribution from patients, especially in Cameroon where more than 70% of health expenditures are incurred by households. This study assessed the direct costs of diagnostic digestive endoscopy, based on indications and patient outcomes in Yaoundé, Cameroon. A retrospective cross-sectional study was conducted, over a period of twelve months in the digestive endoscopy units of two referral health facilities (one private and one public). The sampling exhaustively included the reports of gastroscopies and diagnostic colonoscopies. Direct costs were estimated from expenditures for examination, anaesthesia, biopsy, colonic preparation in the patient's perspective in relation to clinical indications, endoscopies (type of anaesthesia, type of endoscopy, biopsy, results) of gastroscopies and colonoscopies performed. The average total cost was estimated by dividing the overall total cost by the number of patients. The costs were expressed in Central Africa Francs XAF, and US Dollars ($1= 554.24 XAF). Statistical analyses used the non-parametric Mann-Whitney test. Differences at the 5% threshold were considered significant. A total of 1,147 reports met our selection criteria: 754 gastroscopies and 393 diagnostic colonoscopies with an average patient age of 45 years. In gastroscopy, 46.8% were men and 53.2% were women, while in colonoscopy, there were 58.3% men and 41.7% women. The average direct cost of gastroscopy was estimated at 46,981 XAF ($84.77) per patient; while the cost of colonoscopy was 117,692 XAF ($212.35) per patient. The main indications that influenced the overall direct cost of gastroscopy were: pyrosis with 42,000 XAF ($75.7) and melena with 45,000 XAF ($81). The endoscopic findings responsible for a fluctuation in this cost were mainly: bulbar ulcer and absence of lesions, each with 60,000 XAF ($108.11). The overall direct cost of colonoscopy was influenced by indications such as: rectorrragies with 109,000 XAF ($196.4) and abdominal pain with 108,200 XAF ($194.96); as well as by certain results such as: absence of lesions with 108,000 XAF ($194.59) and colonic polyps with 142,000 XAF ($255.86). The study concludes that digestive endoscopy was likely expensive in the study setting. Often some inappropriate indications were posed, such as pyrosis and abdominal pain, thereby contributing to increase the cost of digestive endoscopy. This makes digestive endoscopy financially inaccessible to less well-off patients. The policy implications lies in providing evidence for subsidising the costs of digestive endoscopy as part of universal health coverage benefit package in Cameroon.
| Published in | International Journal of Health Economics and Policy (Volume 10, Issue 3) |
| DOI | 10.11648/j.hep.20251003.11 |
| Page(s) | 77-89 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Direct Cost, Diagnostic Digestive Endoscopy, Gastroscopy, Colonoscopy, Indications, Policy Implications, Universal Health Coverage, Cameroon
Variables | N (%) | |
|---|---|---|
Gastroscopies | Colonoscopies | |
Gender | ||
Men | 353 (46.8) | 229 (58.3) |
Women | 401 (53.2) | 164 (41.7) |
Age (years) | ||
< 20 | 47 (6.2) | 24 (6) |
20-39 | 287 (38.1) | 116 (29.6) |
40-59 | 257 (34.1) | 140 (35.7) |
60-79 | 149 (19.8) | 109 (27.7) |
>80 | 14 (1.9) | 4 (1) |
Variables | n (%) | |
|---|---|---|
Gastroscopies | Colonoscopies | |
Type of anesthesia | ||
Local anesthesia | 734 (97.3) | --- |
Intravenous sedation | 20 (2.7) | 229 (57.3) |
Without anesthesia | --- | 164 (41.7) |
Biopsy | ||
Yes | 581 (77.1) | 85 (21.7) |
No | 173 (22.9) | 298 (75.7) |
Not specified | --- | 10 (2.6) |
Colonic preparation | ||
Fortrans® + Normacol® | --- | 178 (45.2) |
Normacol® | --- | 133 (33.9) |
Fortrans® | --- | 48 (12.2) |
Normacol® + X-prep® | --- | 20 (5.2) |
Senna (X-Prep®) | --- | 4 (0.9) |
Results | n (%) |
|---|---|
Erythematous antritis | 219 (18) |
Erythematous pangastritis | 161 (13.3) |
Erythematous funditis | 109 (9.0) |
Bulbar ulcer | 94 (7.7) |
No lesions | 85 (7.0) |
Congestive pangastritis | 84 (6.9) |
Antral ulcer | 82 (6.8) |
Congestive heart failure | 69 (5.7) |
Congestive funditis | 50 (4.1) |
Esophageal varices | 50 (4.1) |
Esophageal mycoses | 39 (3.2) |
Peptic esophagitis | 34 (2.8) |
Other injuries | 31 (2.5) |
Endobrachyoesophagus | 27 (2.2) |
Fundal ulcer | 19 (1.6) |
Hiatal hernia | 15 (1.2) |
Malignant-appearing gastric tumor | 14 (1.2) |
Pyloric ulcer | 13 (1.1) |
Malignant-appearing esophageal tumor | 12 (1.0) |
Pyloric stenosis | 7 (0.6) |
Results | n (%) |
|---|---|
No lesions | 158 (39.1) |
Hemorrhoids | 69 (17.1) |
Colonic polyps | 42 (10.4) |
Diverticulosis | 30 (7.4) |
Malignant-appearing colorectal tumor | 27 (6.7) |
Colitis | 24 (5.9) |
Recites | 23 (5.7) |
Solitary colon ulcer | 12 (3.0) |
Other injuries | 11 (2.7) |
Anal fissures | 4 (1.0) |
Anal ulcer | 4 (1.0) |
Variables | Average XAF ($) | Percentage% | Minimum XAF ($) | Maximum XAF ($) |
|---|---|---|---|---|
Lab Exam cost | 42,263 (76.2) | 40.2 | 37,000 (66.8) | 45,000 (81.2) |
Cost of possible sedation | 58,047 (104.7) | 55.3 | 29,000 (52.3) | 60,000 (108.3) |
Cost of possible biopsy | 4,718 (8.5) | 4.5 | 3,570 (6.4) | 5,000 (9) |
Cost of gastroscopy | ||||
Without sedation | 46,981 (84.7) | 44.7 | 40,570 (73.2) | 50,000 (90.2) |
With sedation | 105,028 (189.6) | 100 | 69,570 (125.6) | 110,000 (198.5) |
Variables | Average XAF ($) | Percentage% | Minimum XAF ($) | Maximum XAF ($) |
|---|---|---|---|---|
Lab Exam cost | 52,515 (94.8) | 44.6 | 18,750 (33.8) | 70,000 (126.3) |
Cost of possible anesthesia | 56,537 (102) | 48.0 | 29,000 (52.3) | 70,000 (126.3) |
Cost of possible biopsy | 4,471 (8) | 3.8 | 3,750 (6.7) | 5,000 (9) |
Cost of colonic preparation | 4,169 (7.5) | 3.5 | 1,500 (2.7) | 8,200 (14.8) |
Cost of colonoscopy | ||||
Without sedation | 61,402 (110.8) | 52 | 24,000 (43.3) | 83,200 (150.2) |
With sedation | 117,692 (212.3) | 100 | 53,000 (95.7) | 153,200 (276.5) |
Indications | Lab Exam cost XAF ($) | Cost of sedation XAF ($) | Biopsy cost XAF ($) | Overall cost of gastroscopy XAF ($) |
|---|---|---|---|---|
Heartburn | 2,579,031 (4,655) | 3,030,943 (5,471) | 201,222 (363.2) | 5,811,196 (10,485) |
Melena | 2,388,984 (4,312) | 2,704,280 (4,881) | 204,516 (369) | 5,297,780 (9,558) |
Weight loss | 764,000 (1,379) | --- | 72,500 (130.8) | 836,000 (1,509) |
Indications | Lab Exam cost XAF ($) | Cost of anesthesia XAF ($) | Biopsy cost XAF ($) | Cost of colonic preparation XAF ($) |
|---|---|---|---|---|
Rectorrhagia | 2,828,504 (5,105.6) | 2,713,176 (4,897.4) | 206,488 (372.7) | 220,586 (398.2) |
Melena | 242,000 (436.8) | 241,000 (435) | 20,000 (36.1) | 17,200 (31) |
Chronic diarrhea | 820,005 (1,480.1) | 669,400 (1,208.3) | 47,505 (85.7) | 67,800 (122.4) |
Lower abdominal pain | 1,763,510 (3,183.2) | 1,749,300 (3,157.6) | 133,735 (241.4) | 130,305 (235.2) |
Iron deficiency anemia | 238,000 (429.6) | 187,500 (338.4) | --- | 12,600 (22.7) |
Abdominal mass | 276,003 (498.2) | 312,400 (564) | 31,752 (57.3) | 21,602 (39) |
Results | Lab Exam cost XAF ($) | Cost of sedation XAF ($) | Biopsy cost XAF ($) | Overall cost of gastroscopy XAF ($) |
|---|---|---|---|---|
No lesions | 3,673,020 (6,630) | 4,275,079 (7,716) | 337,535 (609) | 8,285,634 (14,956) |
Congestive heart failure | 2,824,998 (5,099) | --- | 228,735 (412) | 3,053,733 (5,512) |
Bulbar ulcer | 3,910,024 (7,057) | 4,553,570 (8,219) | 299,954 (541) | 8,763,548 (15,818) |
Congestive funditis | 2,194,000 (3,960) | 2,383,000 (4,301) | 212,500 (383) | 4,789,500 (8,645) |
Esophageal varices | 2,026,000 (3,657) | --- | 240,000 (433) | 2,266,000 (4,090) |
Congestive pangastritis | 3,468,024 (6,260) | 4,026,938 (7,268) | 292,488 (528) | 7,787,450 (14,056) |
Pyloric ulcer | 513,006 (926) | --- | 51,753 (93) | 564,759 (1,019) |
Endobrachyoesophagus | 1,125,000 (2,030) | --- | 125,000 (225) | 1,250,000 (2,256) |
Results | Lab Exam cost XAF ($) | Cost of anesthesia XAF ($) | Biopsy cost XAF ($) | Cost of colonic preparation XAF ($) | Cost of colonoscopy XAF ($) |
|---|---|---|---|---|---|
No lesions | 2,454,744 (4,431) | 1,561,860 (2,819) | 158,010 (285) | 190,716 (344) | 4,365,330 (7,879) |
Colonic polyps | 576,000 (1,039) | 526,580 (950) | 28,998 (52) | 42,399 (76) | 1,173,977 (2,119) |
Diverticulosis | 543,996 (932) | 339,148 (612) | 35,496 (64) | 33,399 (60) | 952,039 (1,718) |
Colonic ulcer | 310,000 (559) | 249,900 (449) | 20,000 (36) | 23,800 (43) | 603,700 (1,089) |
EGD | Esogastroduodenal Endoscopy or Upper Endoscopy |
EPAGE | European Panel on the Appropriateness in Gastroenterolgy Endoscopy |
FMBS | Faculty of Medicine and Biomedical Sciences |
HEREG | Health Economics & Policy Research and Evaluation for Development Results Group |
MST | Minimal Standard Terminology |
XAF | Franc of Central African Country Community |
| [1] | Abdu SM, Assefa EM, Abdu H (2025). Indications and endoscopic findings of upper gastrointestinal diseases in Africa: A systematic review & meta-analysis. PLoS ONE 20(3): e0319854. |
| [2] | Haider SA, Bills GS, Gyawali CP, Laoveeravat P, Miller J, Softic S, Wagh MS, Gabr M. (2023). Direct cost variance analysis of peroral endoscopic myotomy vs heller myotomy for management of achalasia: A tertiary referral center experience. World J Gastrointest Endosc. 2023 Oct 16; 15(10): 593-601. |
| [3] | Crott R. Makris N., Barkun a. and Fallone C (2002). The cost of an upper gastroduodenal endoscopy: An activity-based approach. Canadian journal of gastroenterology = Journal canadien de gastroenterologie 16(7): 473-82. |
| [4] | Yan X, Li X, Chen Y, Ouzhu M, Guo Z, Lyu C, Yang D, Chen H, Xie F, Wu D. (2025). Health economics evaluation of diagnostic strategies for gastroesophageal reflux disease with reflux symptoms in China: a modeling study. BMJ Open. 2025 May 14; 15(5): e093108. |
| [5] | National Institute of Statistics (2024). Results of the 5th Cameroon Household Survey (ECAM5), Press release of April 30, 2024. Yaounde, Cameroon. |
| [6] | Ministry of Public Health (2021). Cameroon National Health Accounts 2018-2019: Final Report. Yaounde, Cameroon. |
| [7] | National Technical Group. Establishment of Universal Health Coverage in Cameroon. Yaoundé: MINSANTE; 2018. |
| [8] | Kohn K, Kosecoff J, Solomon D, Brook H. The Use and Misuse of Upper Gastrointestinal Endoscopy. Annals of internal medicine. Nov 1, 1998; 664 ‑70. |
| [9] | Aabakken L, Rembacken B, LeMoine O, Kuznestsov K, Rey JF, Rosch T et al. Minimal Standard Terminology for gastrointestinal endoscopy 3.0 (MST 3.0). Word Endoscopy Organization (formerly known as OMED). Endoscopy. 2009; 41: 727-8. |
| [10] |
Laté LM, Bouglouga O, Bagny A, Kaaga L, Redah D. Upper gastrointestinal fibroscopy in 2795 patients at the Lomé University Hospital-Campus: specificities according to sex. Pan Afr Med J [Online]. 2014 September [cited 19/12/2019]; 19(262): [19 pages]. Available at URL:
http://www.panafrican-med-journal.com/content/article/19/262/full/ |
| [11] | Ndjitoyap EC, Njoya O, Mballa E, Nsangou MF, Njapom C, Moukouri NE et al. Contribution of endoscopy in lower digestive pathology in Cameroon: analytical study of 720 examinations. Med Afr Noire. 1991; 38: 835-41. |
| [12] | Ndjitoyap EC, Tzeuton C, Mbakop A, Pouepene J, Guemne TA, Njoya O et al. Upper gastrointestinal endoscopy in Cameroon. Analytical study of 4100 examinations. Med Afr Noire. 1990; 37: 453-6. |
| [13] | Eloumou B, Luma N, Noah N, Essomba NE, Malongue A, Manga A et al. Risk factors associated with gastroduodenal lesions in a Douala referral hospital (Cameroon). Med Sante Trop 2016; 26: 104-109. |
| [14] | Assi C, Saoudein K, Ouattara A, Soro D. Total colonoscopy in 2015 in a university hospital in Abidjan: conditions of performance and results. African Journal of Hepato-Gastroenterology. 2017; 11: 1-4. |
| [15] | Ankouane Andoulo F, Kowo M, Ngo Nonga B, Djapa R, Tagni-Sartre M, Njoya O et al. Indications, results and yield of colonoscopy in an unfavorable economic environment: the case of Cameroon. Health Sci Dis [Online]. 2013 November [Cited 28/12/2019]; 14(4): [6 pages]. Available at URL: |
| [16] | Metila D. Contribution of endoscopy in the diagnosis of upper digestive diseases in the city of Yaoundé. [Thesis]. Hepato-Gastroenterology: Yaoundé; 2018. 136 p. |
| [17] | Peytremann-Bridevaux I, Arditi C, Froehlich F, O'Malley J, Fairclough P, Le Moine O, et al. Appropriateness of colonoscopy in Europe (EPAGE II). Iron-deficiency anemia and hematochezia. Endoscopy. 2009; 41(3): 227-33. |
| [18] | Sahai A. V. (2000). Cost-Effectiveness Studies in Endoscopy: Are They Worth it? Endoscopy 2000; 32(12): 986-990. |
| [19] | Di Giulio E, Hassan C, Pickhardt PJ, Zullo A, Laghi A, Kim DH, Iafrate F. (2009). Cost-effectiveness of upper gastrointestinal endoscopy according to the appropriateness of the indication. Scand J Gastroenterol. 2009; 44(4): 491-8. |
| [20] | Hassan C, Di Giulio E, Pickhardt PJ, Zullo A, Laghi A, Kim DH, Iafrate F, Morini S. (2008). Cost effectiveness of colonoscopy, based on the appropriateness of an indication. Clin Gastroenterol Hepatol. 2008 Nov; 6(11): 1231-6. |
| [21] | Sautereau D, Cessot F, Rigaud G. Anesthésie et endoscopie digestive. Encycl Med Chir. (Elsevier Masson, Paris), 1999. 10 p. |
| [22] |
Zullo A, Manta R, De Francesco V, Fiorini G, Hassan C, Vaira D. (2019). Diagnostic yield of upper endoscopy according to appropriateness: A systematic review. Dig Liver Dis. 2019 Mar; 51(3): 335-339.
https://doi.org/10.1016/j.dld.2018.11.029 Epub 2018 Dec 10. |
APA Style
Njoumemi, Z., Ebéké, A. I. K., Ndam, A. W. N., Andoulo, F. A. (2025). Direct Cost Analysis of Diagnostic Digestive Endoscopy Based on Indications and Results in Yaoundé: Policy Implications for Universal Health Coverage in Cameroon. International Journal of Health Economics and Policy, 10(3), 77-89. https://doi.org/10.11648/j.hep.20251003.11
ACS Style
Njoumemi, Z.; Ebéké, A. I. K.; Ndam, A. W. N.; Andoulo, F. A. Direct Cost Analysis of Diagnostic Digestive Endoscopy Based on Indications and Results in Yaoundé: Policy Implications for Universal Health Coverage in Cameroon. Int. J. Health Econ. Policy 2025, 10(3), 77-89. doi: 10.11648/j.hep.20251003.11
AMA Style
Njoumemi Z, Ebéké AIK, Ndam AWN, Andoulo FA. Direct Cost Analysis of Diagnostic Digestive Endoscopy Based on Indications and Results in Yaoundé: Policy Implications for Universal Health Coverage in Cameroon. Int J Health Econ Policy. 2025;10(3):77-89. doi: 10.11648/j.hep.20251003.11
@article{10.11648/j.hep.20251003.11,
author = {Zakariaou Njoumemi and Agnès Ingrid Kpolom Ebéké and Antonin Wilson Ndjitoyap Ndam and Firmin Ankouane Andoulo},
title = {Direct Cost Analysis of Diagnostic Digestive Endoscopy Based on Indications and Results in Yaoundé: Policy Implications for Universal Health Coverage in Cameroon
},
journal = {International Journal of Health Economics and Policy},
volume = {10},
number = {3},
pages = {77-89},
doi = {10.11648/j.hep.20251003.11},
url = {https://doi.org/10.11648/j.hep.20251003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.hep.20251003.11},
abstract = {In low-income countries, the cost of digestive endoscopy procedures is often unknown, yet its understanding is crucial for including them in the universal health coverage benefit package. The management of digestive endoscopy requires substantial financial contribution from patients, especially in Cameroon where more than 70% of health expenditures are incurred by households. This study assessed the direct costs of diagnostic digestive endoscopy, based on indications and patient outcomes in Yaoundé, Cameroon. A retrospective cross-sectional study was conducted, over a period of twelve months in the digestive endoscopy units of two referral health facilities (one private and one public). The sampling exhaustively included the reports of gastroscopies and diagnostic colonoscopies. Direct costs were estimated from expenditures for examination, anaesthesia, biopsy, colonic preparation in the patient's perspective in relation to clinical indications, endoscopies (type of anaesthesia, type of endoscopy, biopsy, results) of gastroscopies and colonoscopies performed. The average total cost was estimated by dividing the overall total cost by the number of patients. The costs were expressed in Central Africa Francs XAF, and US Dollars ($1= 554.24 XAF). Statistical analyses used the non-parametric Mann-Whitney test. Differences at the 5% threshold were considered significant. A total of 1,147 reports met our selection criteria: 754 gastroscopies and 393 diagnostic colonoscopies with an average patient age of 45 years. In gastroscopy, 46.8% were men and 53.2% were women, while in colonoscopy, there were 58.3% men and 41.7% women. The average direct cost of gastroscopy was estimated at 46,981 XAF ($84.77) per patient; while the cost of colonoscopy was 117,692 XAF ($212.35) per patient. The main indications that influenced the overall direct cost of gastroscopy were: pyrosis with 42,000 XAF ($75.7) and melena with 45,000 XAF ($81). The endoscopic findings responsible for a fluctuation in this cost were mainly: bulbar ulcer and absence of lesions, each with 60,000 XAF ($108.11). The overall direct cost of colonoscopy was influenced by indications such as: rectorrragies with 109,000 XAF ($196.4) and abdominal pain with 108,200 XAF ($194.96); as well as by certain results such as: absence of lesions with 108,000 XAF ($194.59) and colonic polyps with 142,000 XAF ($255.86). The study concludes that digestive endoscopy was likely expensive in the study setting. Often some inappropriate indications were posed, such as pyrosis and abdominal pain, thereby contributing to increase the cost of digestive endoscopy. This makes digestive endoscopy financially inaccessible to less well-off patients. The policy implications lies in providing evidence for subsidising the costs of digestive endoscopy as part of universal health coverage benefit package in Cameroon.},
year = {2025}
}
TY - JOUR T1 - Direct Cost Analysis of Diagnostic Digestive Endoscopy Based on Indications and Results in Yaoundé: Policy Implications for Universal Health Coverage in Cameroon AU - Zakariaou Njoumemi AU - Agnès Ingrid Kpolom Ebéké AU - Antonin Wilson Ndjitoyap Ndam AU - Firmin Ankouane Andoulo Y1 - 2025/07/19 PY - 2025 N1 - https://doi.org/10.11648/j.hep.20251003.11 DO - 10.11648/j.hep.20251003.11 T2 - International Journal of Health Economics and Policy JF - International Journal of Health Economics and Policy JO - International Journal of Health Economics and Policy SP - 77 EP - 89 PB - Science Publishing Group SN - 2578-9309 UR - https://doi.org/10.11648/j.hep.20251003.11 AB - In low-income countries, the cost of digestive endoscopy procedures is often unknown, yet its understanding is crucial for including them in the universal health coverage benefit package. The management of digestive endoscopy requires substantial financial contribution from patients, especially in Cameroon where more than 70% of health expenditures are incurred by households. This study assessed the direct costs of diagnostic digestive endoscopy, based on indications and patient outcomes in Yaoundé, Cameroon. A retrospective cross-sectional study was conducted, over a period of twelve months in the digestive endoscopy units of two referral health facilities (one private and one public). The sampling exhaustively included the reports of gastroscopies and diagnostic colonoscopies. Direct costs were estimated from expenditures for examination, anaesthesia, biopsy, colonic preparation in the patient's perspective in relation to clinical indications, endoscopies (type of anaesthesia, type of endoscopy, biopsy, results) of gastroscopies and colonoscopies performed. The average total cost was estimated by dividing the overall total cost by the number of patients. The costs were expressed in Central Africa Francs XAF, and US Dollars ($1= 554.24 XAF). Statistical analyses used the non-parametric Mann-Whitney test. Differences at the 5% threshold were considered significant. A total of 1,147 reports met our selection criteria: 754 gastroscopies and 393 diagnostic colonoscopies with an average patient age of 45 years. In gastroscopy, 46.8% were men and 53.2% were women, while in colonoscopy, there were 58.3% men and 41.7% women. The average direct cost of gastroscopy was estimated at 46,981 XAF ($84.77) per patient; while the cost of colonoscopy was 117,692 XAF ($212.35) per patient. The main indications that influenced the overall direct cost of gastroscopy were: pyrosis with 42,000 XAF ($75.7) and melena with 45,000 XAF ($81). The endoscopic findings responsible for a fluctuation in this cost were mainly: bulbar ulcer and absence of lesions, each with 60,000 XAF ($108.11). The overall direct cost of colonoscopy was influenced by indications such as: rectorrragies with 109,000 XAF ($196.4) and abdominal pain with 108,200 XAF ($194.96); as well as by certain results such as: absence of lesions with 108,000 XAF ($194.59) and colonic polyps with 142,000 XAF ($255.86). The study concludes that digestive endoscopy was likely expensive in the study setting. Often some inappropriate indications were posed, such as pyrosis and abdominal pain, thereby contributing to increase the cost of digestive endoscopy. This makes digestive endoscopy financially inaccessible to less well-off patients. The policy implications lies in providing evidence for subsidising the costs of digestive endoscopy as part of universal health coverage benefit package in Cameroon. VL - 10 IS - 3 ER -
Department of Public Health, Faculty of Medicine and Biomedical Sciences (FMSB), University of Yaoundé 1, Yaounde, Cameroon. Health Economics & Policy Research and Evaluation for Development Results Group (HEREG), Yaounde, Cameroon
Department of Public Health, Faculty of Medicine and Biomedical Sciences (FMSB), University of Yaoundé 1, Yaounde, Cameroon
Department of Internal Medicine, Faculty of Medicine and Biomedical Sciences (FMSB), University of Yaoundé 1, Yaounde, Cameroon. Yaoundé General Hospital, Yaounde, Cameroon
Department of Internal Medicine, Faculty of Medicine and Biomedical Sciences (FMSB), University of Yaoundé 1, Yaounde, Cameroon. Yaoundé General Hospital, Yaounde, Cameroon
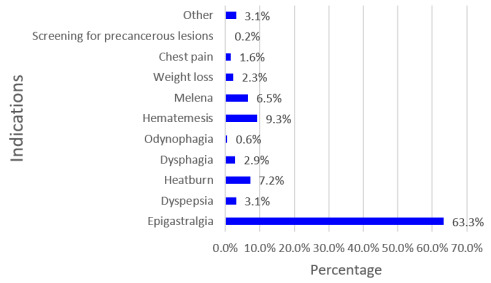
Figure 1. Indications found in gastroscopy.
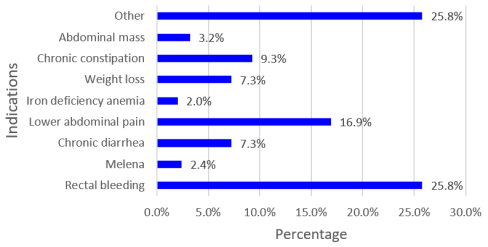
Figure 2. Indications found in colonoscopy.
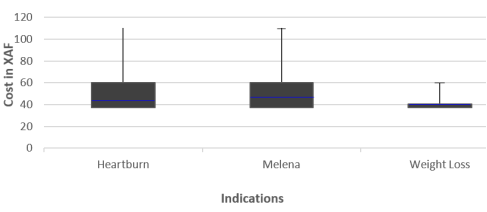
Figure 3. Diagram of indications influencing the cost of diagnostic gastroscopy.
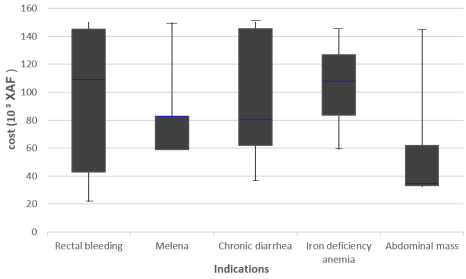
Figure 4. Diagram of indications significantly influencing the cost of colonoscopy.
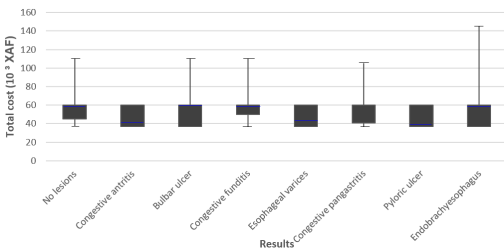
Figure 5. Diagram of results significantly influencing the cost of gastroscopy.

Figure 6. Diagram of results significantly influencing the cost of colonoscopy.
Information

