Abstract
Introduction: Open Tibial Shaft Fractures (TSF) are the most commonly encountered injury type in Cameroon. External fixation, relatively unfamiliar in Cameroon, helps prevent its complications. Objectives: The objective of this study was to evaluate the outcomes of the treatment of TSF using external fixation in Cameroon. Materials and Methods: Patients operated at Laquintinie and Edea Regional Hospital (ERH) with an external fixator (EF) for TSF were followed up from 2018 to 2022. Circumstances of the trauma, anatomo-clinical lesions, types of management, complications, and duration of fixator maintenance were assessed. Results: 161 EFs were placed on 144 patients. Of these, 93 (64.6%) were aged between 20 and 49 years with a sex ratio of 2.5/1. Motorcycle crashes were involved in 68.2% of patients. The fracture involved the middle third in 61 patients (37.9%). It was oblique in 57 patients (35.4%). The injuries were open in 126 (78.3%) cases. The average length of hospital stay was 36.2 days. 122 fractures (75.8%) healed within the expected time, and 21 cases (13.0%) of delayed union were observed. Bone infection was noted in 24 patients (14.9%). The outcome was deemed excellent and good in 122 cases (84.8%). Conclusion: External fixation is effective in managing TSF and is recommended for wider use in Cameroon.
Keywords
Tibia Shaft Fracture, External Fixator, Laquintinie, Edea Regional Hospital
1. Introduction
According to the Cameroon Trauma Registry (CTR), 7605 trauma cases were recorded in four major hospitals (1 central hospital, 3 regional hospitals) in 2017, with 61.2% of these being victims of road accidents
| [1] | Blair, K. J., et al. (2022). Associations between social determinants of health and interpersonal violence-related injury in Cameroon: a cross-sectional study, BMJ Global Health, 7(1), e007220. |
[1]
. The majority of injuries affect the lower limb, with the tibia being the most frequently affected bone
| [2] | Kapend, D. et al. (2022). Infectious complications of long bone fractures operated on at the university clinics of Lubumbashi, 54. |
[2]
. It is known that the most common diaphyseal injury in men is an open fracture of the tibia
| [3] | Bonnevialle, P. (2005). Fractures diaphysaires de l’adulte (fractures pathologiques exclues), EMC - Rhumatologie-Orthopédie, 2(4), 394. |
| [4] | Nana, C. T. et al. (2021). Epidemiological and Clinical Pattern of Open Fractures of Long Bones of the Lower Limbs in the South-West Region of Cameroon: A 5-Year Review, Open Journal of Orthopedics, 11(9), 278. |
[3, 4]
.
The aim of fracture treatment is to achieve timely healing and a return to normal limb activities. This is achieved by restoring the transmission of forces while preserving a favorable biological and mechanical environment for healing. While orthopedic treatments ideally protect the healing physiology, they often entail prolonged immobilization with potential secondary displacement risks. Plate or intramedullary nail osteosynthesis promoting early mobilization, may interfere with healing physiology and increase the risk of infection.
External fixation, where implants are placed away from the fracture site, ensures the alignment of bone fragments and preserves the healing physiology
| [5] | Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58. |
| [6] | Court-Brown, C. M., Wheelwright, E. F., Christie, J., McQueen, M. M. (199). External fixation for type III open tibial fractures, The Journal of Bone & Joint Surgery British Volume, 72-B(5), 801. |
| [7] | Ghiasi, M. S., Chen, J., Vaziri, A., Rodriguez, E. K., Nazarian, A. (2017). Bone fracture healing in mechanobiological modeling: A review of principles and methods, Bone Reports, 6, 87. |
| [8] | Marsh, D. R., Li, G. (1999). The biology of fracture healing: optimising outcome, British Medical Bulletin, 55(4), 856. |
| [9] | Biggi, F. (2002). The Biology of Fracture Healing as Related to Intramedullary Locked Nailing, in Practice of Intramedullary Locked Nails: Scientific Basis and Standard Techniques Recommended by “Association Internationale pour I’Ostéosynthèse Dynamique” (AIOD), I. Kempf, K. S. Leung, A. Grosse, H. J. T. M. Haarman, H. Seidel, et G. Taglang, Éd., Berlin, Heidelberg: Springer, 5. |
| [10] | McKibbin, B. (1978). The biology of fracture healing in long bones, The Journal of Bone & Joint Surgery British Volume, 60-B(2), 150. |
| [11] | Boccaccio, A., Pappalettere, C., Boccaccio, A., Pappalettere, C. Mechanobiology of Fracture Healing: Basic Principles and Applications in Orthodontics and Orthopaedics, in Theoretical Biomechanics, Intech Open, 2011. https://doi.org/10.5772/19420 |
| [12] | Phillips, A. M. (2005). Overview of the fracture healing cascade, Injury, 36(3), Supplement, S5. |
| [13] | Schmal, H., Strohm, P. C., Jaeger, M., Südkamp, N. P. (2011). Flexible Fixation and Fracture Healing: Do Locked Plating ‘Internal Fixators’ Resemble External Fixators?, Journal of Orthopaedic Trauma, 25, S15. |
| [14] | Noordeen, M. H., Lavy, C. B., Shergill, N. S., Tuite, J. D., Jackson, A. M. (1995). Cyclical micromovement and fracture healing, The Journal of Bone & Joint Surgery British Volume, 77-B(4), 645. |
[5-14]
. Its ease of implementation, possible reuse of external components, and system modularity are additional advantages, especially in settings with limited material resources.
For several years, due to the significant influx of trauma cases, external fixation has been adopted as the definitive treatment for all open tibial fractures and some closed fractures at both Laquintinie and the ERH which receive accident victims from major roadways. The objective of the present study was to assess the outcome of treating TSF with an EF in Laquintinie and the ERH over a 5-year period.
2. Patients and Methods
2.1. Study Design
This is a descriptive, cross-sectional study with retrospective data collection carried out in 6 months (From December 1, 2022 to May 31, 2023). The study included medical files of patients who presented with a TSF and treated at Laquintinie and the ERH with EF. These hospitals receive trauma victims from the road axis connecting the two most important cities in Cameroon, Yaoundé and Douala.
2.2. Study Procedure
Variables related to trauma circumstances, clinical and radiographic data were collected with the support of the CTR, a digital platform registering all trauma patients admitted to the hospital. All patient, trauma, surgical intervention, and postoperative follow-up data were recorded. The selected patients underwent preoperative radiography, immediate postoperative radiography, and at least one final outpatient radiography before EF removal. They were contacted by telephone, and appointments were scheduled after verbal and written consent.
Sociodemographic data (age, sex, occupation, address, religion, marital status, etc.) were recorded. Associated injuries were investigated. The presence of preoperative treatment, type of surgery, and complications were noted. Admission time after trauma, time to surgical treatment, length of hospital stay, and duration of EF maintenance were examined. Radiographs were analyzed to determine the location and configuration of the fracture line, pre- and immediate postoperative deformities. Deformities sought in radiographs included frontal angulations (varus, valgus), sagittal (anterocurvatum, recurvatum), rotations, overlaps, and translations. During outpatient visits, radiographs determined the appearance and type of consolidation, such as the presence or absence of periosteal callus, persistence or absence of the fracture line, continuity or interruption of bone trabeculae, and the presence or absence of bone substance loss or osteolysis at the fracture site or around the pins.
The final outcome was classified according to clinical and paraclinical criteria as excellent, good, satisfactory, or poor. The EF was placed using the usual Hoffmann technique, primarily considering the following configurations: half-frame - 1 bar, half-frame - 2 bars, triangle-2 bars, hybrid assembly, or combined with another type of osteosynthesis. All data were collected, coded, and analyzed using SPSS version 26.0 software, and Excel 2010 software was used for graph design.
3. Results
During the study period, 1061 patients were received. Of these, 585 (64.8%) presented with leg trauma and 643 had fractures. Among the 643 fractures, 437 (68.0%) were shaft fractures. Of these, 235 (53.8%) underwent surgery, 102 (23.3%) received orthopedic treatment, 18 (4.1%) died, 23 (5.3%) were transferred, and 59 (13.5%) left against medical advice. Of the 235 patients who underwent surgery, 21 (8.9%) were excluded from the study, 39 (16.6%) were treated with intramedullary nailing, 14 (6.0%) with plate fixation, and 144 (61.3%) with EFs. Among the 144 patients operated on with an EF, 17 (7.2%) had bilateral fractures, totaling 161 EFs placed for TSF.
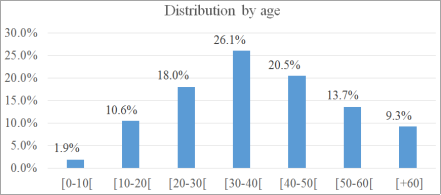
Most patients were between 20 and 49 years old (
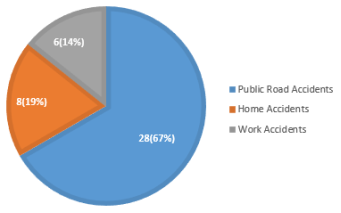
Figure 1). 103 (71.5%) were male, and 41 (28.5%) were female, giving a sex ratio of 2.5/1. Majority of the patients were farmers [10 (23.8%)]. Motorized drivers (motorcycle and car) represented 33.3% (14) of the population. Road traffic crashes accounted for over half of the cases [28 (67%)] (
Figure 2). Motorcycles were involved in 68.2% (60) of accidents (
Table 1). The left side was affected in 52.4% (84) of cases.
Fractures involved the middle diaphysis in 61 cases (37.9%), followed by the distal third in 52 cases (32.3%). Oblique fracture lines [57 (35.4%)] were the most common, followed by transverse lines [31 (19.3%)]). Angulation [16 (52.8%)] was the most represented, followed by overlap [14 (48.4%)]. 21.7% (3) of fractures were non-displaced. The same fracture could present multiple types of deformities, (
Table 2).
A total of 35 cases (21.7%) were closed fractures, while 126 (78.3%) were open, including 47 (29.2%) GA I, 29 (18.0%) GA II, 19 (11.8%) GA IIIA, and 31 (19.3%) GA IIIB. 37 (88.1%) of the studied population was with an open TSF.
Figure 1. Distribution of leg trauma patients by age group.
Figure 2. Distribution by type of accident.
Table 1. Circumstances of occurrence of public road accidents.
Circumstances | Number | Frequency (%) |
Motorcycle-motorcycle | 25 | 28,4% |
Motorcycle-pedestrian | 13 | 14,8% |
Motorcycle-car | 22 | 25,0% |
Car-car | 6 | 6,8% |
Car-pedestrian | 19 | 21,6% |
Car-truck | 3 | 3,4% |
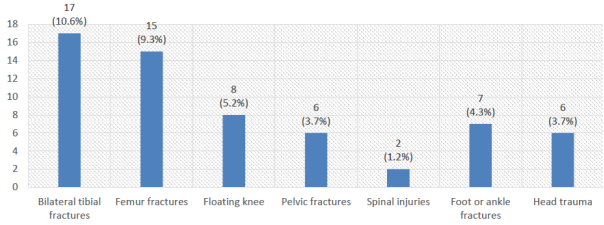
Figure 3. Associated bone injuries.
Table 2. Location configuration of the fracture line.
| Transverse | Oblique | Spiral | Butterfly Wing | Comminuted | TOTAL | % |
1/3 Proximal | 8 | 25 | 5 | 5 | 5 | 48 | 29,8% |
1/3 Middle | 15 | 15 | 11 | 13 | 7 | 61 | 37,9% |
1/3 Distal | 8 | 17 | 7 | 9 | 11 | 52 | 32,3% |
TOTAL | 31 | 57 | 23 | 27 | 23 | 161 | |
% | 19,3% | 35,4% | 14,3% | 16,8% | 14,3% | | |
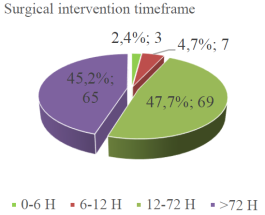
Prevention of thromboembolic disease was achieved by administering low molecular weight heparin. Most patients were managed within 30 to 120 minutes (76.2%). Closed fractures were operated on with an EF if there was an associated hemodynamic instability or other injuries particularly in polytrauma cases. Regarding the operating time, only 3 patients (2.4%) were operated on less than 6 hours after trauma (
Figure 4).
Figure 4. Surgical intervention timeframe.
Hoffmann I (+54.7%) and ASOS (26.7%) fixators were most commonly used. Hoffmann II, which is modular but more expensive, was used in only 30 cases (18.6%). The configurations were mostly half-frame - 2 bars (47.8%) and half-frame - 1 bar (44.1%) (
Table 3). The triangle setup was used to all patients for fractures of the distal third. In the absence of sufficient space at the distal 1/4 of the tibia, this configuration involved bridging the ankle joint with transfixing calcaneal pins and 2 bars. 141 fractures (87.6%) were initially treated with an EF. As for the 20 (12.4%) fractures treated as a second intention, they were either due to the failure of initial osteosynthesis (8), failure of orthopedic treatment (8), or failure after traditional treatment (4).
Immediate complications included compartment syndrome (3.1%), surgical site infection (14.9%), soft tissue inflammation around the pins (7.5%), of which 3.1% required changing the insertion site, while the rest were treated with antibiotics and anti-inflammatories. All cases of osteitis (1.9%) underwent reoperation with the EF in place. Pin tract infection (12.3%) was clinically marked by loosening with suppuration. Some were removed by simple manual traction. Radiographically, osteolysis around the pins was noted. Neuro-algodystrophic syndrome had an 8.1% prevalence in the present study. The average length of hospital stay was 36.2 days (5 weeks 2 days) with a median of 20.0 days. 122 fractures where (75.8%) consolidated within the expected time. 21 fractures (13.0%) progressed to delayed union. There were 18 cases (11.2%) of non-union.
Most EF were removed between 12 and 20 weeks (
Table 4), and mainly during outpatient visits. Over half of the patients (59.7%) were reviewed between 3 and 6 months after discharge. Most patients were not seen after EF removal. The final outcome was excellent in 45 cases (31.3%), good in 77 cases (53.5%), satisfactory in 11 cases (7.6%), and poor in 11 cases (7.6%). These results consider clinical, radiographic data, and patient assessment. Joint assessment of the knee and ankle was normal in all cases where the fracture had healed. There were 9 cases (5.6%) of angular deviation exceeding 5° in the frontal plane and 6 cases (3.7%) in the sagittal plane. A limb length inequality of less than 2cm was found in 7 patients (4.3%), which did not lead to limping.
Table 3. Configuration and type of assembly.
Configuration Type of Fixator | 1/2 Frame 1 Bar | 1/2 Frame 2 Bars | Triangle | Total | Frequency (%) |
AO | 43 | 0 | 0 | 43 | 26,7% |
Hoffmann I | 28 | 47 | 13 | 88 | 54,7% |
1 Bar | 28 | 0 | 0 | 28 | 31,8% |
2 Bars | 0 | 47 | 13 | 60 | 68,2% |
Hoffmann II | 0 | 30 | 0 | 30 | 18,6% |
| 71 | 77 | 13 | 161 | 100,0% |
| 44,1% | 47,8% | 8,1% | 100,0% | |
Table 4. The timeframe for EF removal.
AMOS in weeks | Number | Frequency (%) |
[8-12] | 13 | 9,0% |
[12-16] | 49 | 34,0% |
[16-20] | 73 | 50,7% |
[20-24] | 6 | 4,2% |
[24-28] | 3 | 2,1% |
The first radiograph to check the state of consolidation was taken within an average of 3 months. These x-rays corresponded to the last consultation. A good state of consolidation has been observed in 33 (78.6%) patients and a poor state in 09 (21.4%) patients. Removal of the EF was done in most cases [23 (54.7%)] between 20 and 24 weeks. The average time to consolidation was 5.2 ± 1.2 months. AMOS was performed in most cases [35 (92.8%)] without any complications. The removal of the EF was done on the basis of radiological criteria: presence of a periosteal callus bridging the fracture (66.7%). In a few cases, the patient's wishes [8 (19%)] and infection at the pin implantation site [6 (14.3%)] were the indications for ablation. 37 EF were removed without anesthesia and 5 were removed in the operating room: child (N=2), pain in adults (N=1) and apprehension (N=2). In 33.3% (N=14) of cases, post AMOS treatment was instituted. Infection of cards was the most common indication [5 (35.7%)] followed by the patient's wishes [4 (28.6%)]. We found treatment failure in 3 patients (21.4%). Blisters were found in 12 (28.6%) patients. In 5 (11.9%) patients, compartment syndrome and wound infection have been observed. The superficial peroneal nerve lesion was found in 1 (2.4%) patient. 23 (54.7%) patients developed late complications. The most common complication was osteitis [8 (34.8%)], followed by malunion [7 (30.4%)]. Pin infections were treated with local dressings and oral cloxacylline. One (01) case required hospitalization for IV treatment. Only 2 cases required changing the files before consolidation. In this study, 33.3% (14) of surgeons qualified the treatment results as very good, while 57.7% (24) of patients found the treatment good. Some surgeons [9 (21.4%)] and patients [3 (7.2%)] found the treatment bad. Any factor influencing the occurrence of complications has not been found. No statistically significant difference was found between age, sex, mechanism of injury, affected side, type of fixator, number of screws used and occurrence of late complications.
4. Discussion
Statistical analysis of sociodemographic data has shown that the majority of patients were young subjects with an average age of 39.5± 16.2 years. This result is greater than the ones of Mwafulirwa et al. (34.6 years)
| [15] | Mwafulirwa K, Munthali R, Ghosten I, et al. Epidemiology of Open Tibia fractures presenting to a tertiary referral centre in Southern Malawi: a retrospective study. Mal Med J 2022; 34: 118–122. |
[15]
, Najeb et al. (34.6 years)
| [16] | Najeb Y, Abkari I, Massous A, et al. Resultats du traitement des fractures de jambe par un fixateur externe low cost d’adaptation locale. Rev Maroc Chir Ortho Traumato 2008; 36: 14–7. |
[16]
, Banza et al. (33.4 years)
| [5] | Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58. |
[5]
and Kombate et al. (38 years)
| [17] | Kombate NK, Walla A, Akloa K, et al. Epidemiology of open limb fractures in a country with low-income. Open Journal of Orthopedics 2017; 7: 356–361. |
[17]
. This can be due to the fact that (30-40) years old is the most active age group in Cameroon. Most people at this age have responsibilities and must meet multiple financial needs by leaving their homes. Men represented 71.4% of the study population with a sex ratio equal to 2/1. This male predominance is also reported by Mwafulirwa et al. (82%)
| [15] | Mwafulirwa K, Munthali R, Ghosten I, et al. Epidemiology of Open Tibia fractures presenting to a tertiary referral centre in Southern Malawi: a retrospective study. Mal Med J 2022; 34: 118–122. |
[15]
in Malawi, Nana et al. (75.4%)
| [10] | McKibbin, B. (1978). The biology of fracture healing in long bones, The Journal of Bone & Joint Surgery British Volume, 60-B(2), 150. |
[10]
in Cameroon, Kombate et al. (73.6 %)
| [17] | Kombate NK, Walla A, Akloa K, et al. Epidemiology of open limb fractures in a country with low-income. Open Journal of Orthopedics 2017; 7: 356–361. |
[17]
in Togo and Banza et al. (73.8%)
| [5] | Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58. |
[5]
in Democratic Republic of Congo. The low representation of the female sex (28.6%) was due to the fact that the present study took place in a semi-urban area, and also most of the women residing there engage much more in household activities.
Depending on the circumstance of occurrence, public road accidents were the major accident types (66.7%) which cause TSF. This result is in accordance to that of Banza et al. (88.64%)
| [5] | Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58. |
[5]
; Kombate et al. (73.5%)
| [17] | Kombate NK, Walla A, Akloa K, et al. Epidemiology of open limb fractures in a country with low-income. Open Journal of Orthopedics 2017; 7: 356–361. |
[17]
, Magoumou et al. (86.7%). Road accidents were the main circumstance for the occurrence of fractures in this study because the city of Edea is a crossroads for 03 axes, which leads to the presence of vehicles traveling at high speed. In addition, drivers often recurring non-compliance with the highway code by drivers and the presence of two-wheeled motorized vehicles constitute a contributing factor to the occurrence of road accidents.
Direct shock was the most common mechanism of injury (64.3%). This result is similar to those of Banza et al. (81.8%) in the Democratic Republic of Congo and Kombate et al. (61.2%) in Togo. These results were due to the predominance of road accidents as the occurrence circumstance. The left side was the most affected in this study [22 (52.4%)]. For instance, Najeb et al.
| [16] | Najeb Y, Abkari I, Massous A, et al. Resultats du traitement des fractures de jambe par un fixateur externe low cost d’adaptation locale. Rev Maroc Chir Ortho Traumato 2008; 36: 14–7. |
[16]
found a predominance to the right side in Morocco in 2008. The difference can be due to the fact that automobiles in Cameroon have the driver's side located on the left and also by the configuration of Cameroon’s roads where the curb is on the right, which helps protect the right side.
The median time between the accident and consultation at ERH emergency room was 3 hours. This delay could be due to the fact that the place where the accidents occurred was not always close to ERH. The delay in consultation after an open fracture being a factor of poor prognosis in the future, the rule of 6 hours post-trauma for carrying out surgical debridement to avoid infection has been considered crucial in the prevention of infection
| [18] | Court-Brown CM, Bugler KE, Clement ND, et al. The epidemiology of open fractures in adults. A 15-year review. Injury 2012; 43: 891–897. |
[18]
. In their study, Nana et al. found that the majority of patients (53.5%) were presented to the hospital after 6 hours
| [10] | McKibbin, B. (1978). The biology of fracture healing in long bones, The Journal of Bone & Joint Surgery British Volume, 60-B(2), 150. |
[10]
. The present study indicates 11 polytraumatized patients based on statistical analysis including Cranio-encephalic trauma (11.9%), femur fracture (9.5%), contralateral leg injury (4.7%), maxillofacial trauma (7.1%) and thoracic contusion (4. 7%). This result is too small comparing to that of Magoumou et al.
| [19] | Magoumou A, El Andaloussi Y, Fahsi S, et al. Time management of open lower-leg fractures in Morocco. Open Journal of Emergency Medicine; 2014. |
[19]
who obtained 6 cases in Morocco in 2014, including cranial injuries (40), thoracic injuries (11) and other fractures (9). Banza et al in 2022 found no associated lesion (38.64%). Among the associated injuries found, cranioencephalic trauma was predominant (34.10%) followed by femur fracture (9.10%)
| [5] | Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58. |
[5]
.
In relation to the skin lesions, a predominance of open GAII fractures in 12 patients (28.6%) was observed, followed by GA3B in 11 patients (26.2%) and GA3A in 8 patients (19%). GA1 open fractures were the least represented (7.2%). Nana et al. observed in their study that the majority of open tibia fractures were GA2 [46 (23.6%)] and GA3 including 3A [76 (39%)] and 3B [56 (28.7%)]
| [10] | McKibbin, B. (1978). The biology of fracture healing in long bones, The Journal of Bone & Joint Surgery British Volume, 60-B(2), 150. |
[10]
. Which is close to the results obtained in this study. The latter could be explained by the fact that direct shock is the cause of high-level trauma and this was the most common mechanism of injury found in the study area. Some Authors like Mwafulirwa et al.
| [15] | Mwafulirwa K, Munthali R, Ghosten I, et al. Epidemiology of Open Tibia fractures presenting to a tertiary referral centre in Southern Malawi: a retrospective study. Mal Med J 2022; 34: 118–122. |
[15]
obtained different results. Those results are the following GA2 [20 (33.3%)], GA1 [19 (31.2%)] and, GA3:3A [8 (13.3%)], 3B [13 (21.7%)].
Depending on the fracture displacement on the radiographic images, angulation was the most represented deformation (38.1%). Translation was found in 19% of cases and rotation in 2.4% of cases. 7.1% of fractures had no deformation. For instance, in their study, Banza et al. observed a predominance for rotation.
The average treatment time in the operating room was 106.8 ± 79.3 hours or 4.5 days. This could be explained by the lack of financial means delaying treatment in one hand and the waiting time for the arrival of sick guards for certain patients in the other hand. Likely, Tafsir et al.
| [12] | Phillips, A. M. (2005). Overview of the fracture healing cascade, Injury, 36(3), Supplement, S5. |
[12]
found an average treatment time of 4.5 days in Guinea Conakry in 2022. For instance, these results seems smaller than that of Monka et al.
| [20] | Monka M, Mandavo CM, Zengui Z, et al. Traitement par fixateur externe des fractures ouvertes des membres: à propos de 38 cas. Health Sciences and Disease; 18. |
[20]
who reported an average delay of 5 days in Congo Brazzaville in 2017. All patients were treated openly. This method of treatment has been chosen as similar as did authors of Ref.
| [21] | Junior MM, Daddy-Gratien BA, Roger AK, et al. Indications du fixateur externe aux Cliniques Universitaires de Kisangani, République Démocratique du Congo. |
[21]
due to the anatomical type of the fracture which, in the majority were open fractures, and the need to obtain a perfect reduction. Another reason was the lack of equipment allowing the use of other method.
EF type AO (47.6%) and HOFFMANN I (52.4%) were the most used in in this study. This could be explained by the fact that these 02 types of fixators are the most available in Laquintinie and ERH. Tafsir et al in 2022 found these same types of EF in their study
| [12] | Phillips, A. M. (2005). Overview of the fracture healing cascade, Injury, 36(3), Supplement, S5. |
[12]
. In contrast, Layes et al.
| [22] | Layes T, Terna T, Oumar SC, et al. Traitement des fractures ouvertes des membres par fixateur externe a l’hopital de sikasso (Mali). Revue Africaine de Chirurgie et Specialites; 12. |
[22]
found that the EF Orthofix was the most used in Mali in 2018. At ERH, the majority of patients were not kept hospitalized throughout the duration of treatment. The average length of stay for patients was 12.2±6.4 weeks. This is due to the low economic level of the majority of the above mentionned patients. Layes et al.
| [22] | Layes T, Terna T, Oumar SC, et al. Traitement des fractures ouvertes des membres par fixateur externe a l’hopital de sikasso (Mali). Revue Africaine de Chirurgie et Specialites; 12. |
[22]
found a minimum duration of hospitalization of 39.8 days, or 5.6 weeks in 2018 in Mali in 2018. Junior et al.
| [21] | Junior MM, Daddy-Gratien BA, Roger AK, et al. Indications du fixateur externe aux Cliniques Universitaires de Kisangani, République Démocratique du Congo. |
[21]
in Congo in 2022 showed that most of patients, 84.16%, spent more than 60 days in hospital.
23 patients developed late complications (54.7%) and 45.3% had a favorable outcome without complications. The most common complication was osteitis (34.8%), followed by malunion (30.4%). The explanation which arise from this result is poverty and sometimes even an absence of rigorous post-operative monitoring (poor dressings, early mobilization, traditional monitoring) and lack of financial resources. The length of stay at the ERH could also be a factor favoring the occurrence of these complications.
The EF was maintained throughout the consolidation. Removal of the EF in general was done according to the clinical and radiological criteria of consolidation and was carried out between 12 and 20 weeks for most patients. In a few cases, the patient's wishes (19%) and the infection located on the orifices of the plugs (14.3%) were the indications for ablation. A mean time to consolidation of 5.2 ± 1.2 months was found. It was very difficult for us to compare this period to the periods indicated by other authors because the consolidation criteria are variable and often poorly specified. AMOS was performed in most cases without any complications. Unlikely, it was not possible to assume that the infection of the screws observed in this study and in the series of other authors consulted could perhaps be explained by the insufficiency of post-operative care at the level of the screw orifices
| [20] | Monka M, Mandavo CM, Zengui Z, et al. Traitement par fixateur externe des fractures ouvertes des membres: à propos de 38 cas. Health Sciences and Disease; 18. |
[20]
.
5. Conclusion
The present study found road traffic crashes to be the most abundant injury mechanism among trauma patients in Douala and Edea. In managing the resultant TSF, the Hoffmann EF was the most used. The treatment outcomes were not very good with more than half of patients developing late complications. There is needs to be further training of trauma personnel in the application of EFs to ensure better outcomes.
Abbreviations
ASOS | Association for the Study of Osteosynthesis |
EF | External Fixator |
EFs | External Fixators |
GA | Gustilo-Anderson |
ROSE | Removal of Osteosynthesis Equipment |
SPSS | Statistical Package for Social Sciences |
TSF | Tibial Shaft Fracture |
Author Contributions
All authors made significant contributions to the conceptualization, design, data collection, data analysis, manuscript writing and editing, manuscript translation and proofread. JG Tsiagadigui, BM Mba Wolle, T Nana, L Fonkoue, and OK Muluem conceptualized and designed the study. JG Tsiagadigui and BM Mba Wolle designed the data collection tools and conducted the study. JG Tsiagadigui, CM Ekengoue, MAN Yamben, and T Nana conducted manuscript writing and editing, and manuscript translation and proofread. J Bahebeck and MA Sosso gave overall guidance for the study. All the authors gave final approval to the manuscript for journal submission and are responsible for the content of the manuscript.
Ethical Consideration
Ethical clearance was obtained from the Institutional review board of the University of Douala and the heads of the Higher Institute of Medical Technology (HIMT). Administrative approval was obtained from both Laquintinie and ERH.
Selection Criteria
Patients with a TSF operated on using an EF and who had at least one postoperative consultation were included in the study. Patients with metaphyseal or epiphyseal tibial fractures, those not followed-up, or those with incomplete records were excluded from the study.
Data Availability Statement
The data for this study are not publicly available due to the restrictions from the University of Douala and the Higher Institute of Medical Technology (HIMT) for posting of public data.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Blair, K. J., et al. (2022). Associations between social determinants of health and interpersonal violence-related injury in Cameroon: a cross-sectional study, BMJ Global Health, 7(1), e007220.
|
| [2] |
Kapend, D. et al. (2022). Infectious complications of long bone fractures operated on at the university clinics of Lubumbashi, 54.
|
| [3] |
Bonnevialle, P. (2005). Fractures diaphysaires de l’adulte (fractures pathologiques exclues), EMC - Rhumatologie-Orthopédie, 2(4), 394.
|
| [4] |
Nana, C. T. et al. (2021). Epidemiological and Clinical Pattern of Open Fractures of Long Bones of the Lower Limbs in the South-West Region of Cameroon: A 5-Year Review, Open Journal of Orthopedics, 11(9), 278.
|
| [5] |
Lavini et al. F. (2014). Temporary bridging external fixation in distal tibial fracture, Injury, 45, S58.
|
| [6] |
Court-Brown, C. M., Wheelwright, E. F., Christie, J., McQueen, M. M. (199). External fixation for type III open tibial fractures, The Journal of Bone & Joint Surgery British Volume, 72-B(5), 801.
|
| [7] |
Ghiasi, M. S., Chen, J., Vaziri, A., Rodriguez, E. K., Nazarian, A. (2017). Bone fracture healing in mechanobiological modeling: A review of principles and methods, Bone Reports, 6, 87.
|
| [8] |
Marsh, D. R., Li, G. (1999). The biology of fracture healing: optimising outcome, British Medical Bulletin, 55(4), 856.
|
| [9] |
Biggi, F. (2002). The Biology of Fracture Healing as Related to Intramedullary Locked Nailing, in Practice of Intramedullary Locked Nails: Scientific Basis and Standard Techniques Recommended by “Association Internationale pour I’Ostéosynthèse Dynamique” (AIOD), I. Kempf, K. S. Leung, A. Grosse, H. J. T. M. Haarman, H. Seidel, et G. Taglang, Éd., Berlin, Heidelberg: Springer, 5.
|
| [10] |
McKibbin, B. (1978). The biology of fracture healing in long bones, The Journal of Bone & Joint Surgery British Volume, 60-B(2), 150.
|
| [11] |
Boccaccio, A., Pappalettere, C., Boccaccio, A., Pappalettere, C. Mechanobiology of Fracture Healing: Basic Principles and Applications in Orthodontics and Orthopaedics, in Theoretical Biomechanics, Intech Open, 2011.
https://doi.org/10.5772/19420
|
| [12] |
Phillips, A. M. (2005). Overview of the fracture healing cascade, Injury, 36(3), Supplement, S5.
|
| [13] |
Schmal, H., Strohm, P. C., Jaeger, M., Südkamp, N. P. (2011). Flexible Fixation and Fracture Healing: Do Locked Plating ‘Internal Fixators’ Resemble External Fixators?, Journal of Orthopaedic Trauma, 25, S15.
|
| [14] |
Noordeen, M. H., Lavy, C. B., Shergill, N. S., Tuite, J. D., Jackson, A. M. (1995). Cyclical micromovement and fracture healing, The Journal of Bone & Joint Surgery British Volume, 77-B(4), 645.
|
| [15] |
Mwafulirwa K, Munthali R, Ghosten I, et al. Epidemiology of Open Tibia fractures presenting to a tertiary referral centre in Southern Malawi: a retrospective study. Mal Med J 2022; 34: 118–122.
|
| [16] |
Najeb Y, Abkari I, Massous A, et al. Resultats du traitement des fractures de jambe par un fixateur externe low cost d’adaptation locale. Rev Maroc Chir Ortho Traumato 2008; 36: 14–7.
|
| [17] |
Kombate NK, Walla A, Akloa K, et al. Epidemiology of open limb fractures in a country with low-income. Open Journal of Orthopedics 2017; 7: 356–361.
|
| [18] |
Court-Brown CM, Bugler KE, Clement ND, et al. The epidemiology of open fractures in adults. A 15-year review. Injury 2012; 43: 891–897.
|
| [19] |
Magoumou A, El Andaloussi Y, Fahsi S, et al. Time management of open lower-leg fractures in Morocco. Open Journal of Emergency Medicine; 2014.
|
| [20] |
Monka M, Mandavo CM, Zengui Z, et al. Traitement par fixateur externe des fractures ouvertes des membres: à propos de 38 cas. Health Sciences and Disease; 18.
|
| [21] |
Junior MM, Daddy-Gratien BA, Roger AK, et al. Indications du fixateur externe aux Cliniques Universitaires de Kisangani, République Démocratique du Congo.
|
| [22] |
Layes T, Terna T, Oumar SC, et al. Traitement des fractures ouvertes des membres par fixateur externe a l’hopital de sikasso (Mali). Revue Africaine de Chirurgie et Specialites; 12.
|
Cite This Article
-
APA Style
Tsiagadigui, J. G., Wolle, B. M. M., Nana, T., Fonkoue, L., Muluem, O. K., et al. (2024). External Fixation of Tibial Shaft Fractures in Cameroon-Central Africa. International Journal of Clinical and Experimental Medical Sciences, 10(2), 17-24. https://doi.org/10.11648/j.ijcems.20241002.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Tsiagadigui, J. G.; Wolle, B. M. M.; Nana, T.; Fonkoue, L.; Muluem, O. K., et al. External Fixation of Tibial Shaft Fractures in Cameroon-Central Africa. Int. J. Clin. Exp. Med. Sci. 2024, 10(2), 17-24. doi: 10.11648/j.ijcems.20241002.11
Copy
|
Download
AMA Style
Tsiagadigui JG, Wolle BMM, Nana T, Fonkoue L, Muluem OK, et al. External Fixation of Tibial Shaft Fractures in Cameroon-Central Africa. Int J Clin Exp Med Sci. 2024;10(2):17-24. doi: 10.11648/j.ijcems.20241002.11
Copy
|
Download
-
@article{10.11648/j.ijcems.20241002.11,
author = {Jean Gustave Tsiagadigui and Berna Marquise Mba Wolle and Théophile Nana and Loïc Fonkoue and Olivier Kennedy Muluem and Clautaire Mwebi Ekengoue and Marie-Ange Ngo Yamben and Jean Bahebeck and Maurice Aurélien Sosso},
title = {External Fixation of Tibial Shaft Fractures in Cameroon-Central Africa
},
journal = {International Journal of Clinical and Experimental Medical Sciences},
volume = {10},
number = {2},
pages = {17-24},
doi = {10.11648/j.ijcems.20241002.11},
url = {https://doi.org/10.11648/j.ijcems.20241002.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcems.20241002.11},
abstract = {Introduction: Open Tibial Shaft Fractures (TSF) are the most commonly encountered injury type in Cameroon. External fixation, relatively unfamiliar in Cameroon, helps prevent its complications. Objectives: The objective of this study was to evaluate the outcomes of the treatment of TSF using external fixation in Cameroon. Materials and Methods: Patients operated at Laquintinie and Edea Regional Hospital (ERH) with an external fixator (EF) for TSF were followed up from 2018 to 2022. Circumstances of the trauma, anatomo-clinical lesions, types of management, complications, and duration of fixator maintenance were assessed. Results: 161 EFs were placed on 144 patients. Of these, 93 (64.6%) were aged between 20 and 49 years with a sex ratio of 2.5/1. Motorcycle crashes were involved in 68.2% of patients. The fracture involved the middle third in 61 patients (37.9%). It was oblique in 57 patients (35.4%). The injuries were open in 126 (78.3%) cases. The average length of hospital stay was 36.2 days. 122 fractures (75.8%) healed within the expected time, and 21 cases (13.0%) of delayed union were observed. Bone infection was noted in 24 patients (14.9%). The outcome was deemed excellent and good in 122 cases (84.8%). Conclusion: External fixation is effective in managing TSF and is recommended for wider use in Cameroon.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - External Fixation of Tibial Shaft Fractures in Cameroon-Central Africa
AU - Jean Gustave Tsiagadigui
AU - Berna Marquise Mba Wolle
AU - Théophile Nana
AU - Loïc Fonkoue
AU - Olivier Kennedy Muluem
AU - Clautaire Mwebi Ekengoue
AU - Marie-Ange Ngo Yamben
AU - Jean Bahebeck
AU - Maurice Aurélien Sosso
Y1 - 2024/08/15
PY - 2024
N1 - https://doi.org/10.11648/j.ijcems.20241002.11
DO - 10.11648/j.ijcems.20241002.11
T2 - International Journal of Clinical and Experimental Medical Sciences
JF - International Journal of Clinical and Experimental Medical Sciences
JO - International Journal of Clinical and Experimental Medical Sciences
SP - 17
EP - 24
PB - Science Publishing Group
SN - 2469-8032
UR - https://doi.org/10.11648/j.ijcems.20241002.11
AB - Introduction: Open Tibial Shaft Fractures (TSF) are the most commonly encountered injury type in Cameroon. External fixation, relatively unfamiliar in Cameroon, helps prevent its complications. Objectives: The objective of this study was to evaluate the outcomes of the treatment of TSF using external fixation in Cameroon. Materials and Methods: Patients operated at Laquintinie and Edea Regional Hospital (ERH) with an external fixator (EF) for TSF were followed up from 2018 to 2022. Circumstances of the trauma, anatomo-clinical lesions, types of management, complications, and duration of fixator maintenance were assessed. Results: 161 EFs were placed on 144 patients. Of these, 93 (64.6%) were aged between 20 and 49 years with a sex ratio of 2.5/1. Motorcycle crashes were involved in 68.2% of patients. The fracture involved the middle third in 61 patients (37.9%). It was oblique in 57 patients (35.4%). The injuries were open in 126 (78.3%) cases. The average length of hospital stay was 36.2 days. 122 fractures (75.8%) healed within the expected time, and 21 cases (13.0%) of delayed union were observed. Bone infection was noted in 24 patients (14.9%). The outcome was deemed excellent and good in 122 cases (84.8%). Conclusion: External fixation is effective in managing TSF and is recommended for wider use in Cameroon.
VL - 10
IS - 2
ER -
Copy
|
Download