Abstract
Background: HIV/AIDS and hepatitis B virus (HBV) are two serious global health threats that co-occur and are resistant to antiretroviral therapy (ART). Milions of people worldwide lost their lives to acquired immunodeficiency in 2019.Thus, this study was aimed to evaluate the survival status of patients co-infected with HIV and hepatitis B viruses who are on antiretroviral therapy (HART). Methods: A retrospective cohort study design was conducted. Individuals with HIV-HBV co-infected with HIV mono-infected in six health facilities in Mekelle City from January 2009 to February 2018. The total sample size was 466, of which 94 were HBV exposed and 372 were unexposed for HBV on ART clients. Kaplan-Meier survival and Cox proportional hazard models for survival analysis were used. Data was analyzed using STATA version 14. Result: Of the total patients, 300 (64.3%) were females and most age groups were 15-30 years old, 199 (43%). Over 1960 person years of observation time at risk, 23 (24%) HIV-HBV co-infected and 26 (7%) HIV mono-infected died. In the adjusted analysis, HIV-HBV co-infected group had a 2.53 times increased hazard of death (aHR: 2.52; 95% CI: 1.31-4.85) than HIV mono-infected. Conclusion: In this cohort study, mortality is higher in the HIV-HBV co-infected group. Hence, special attention shall be given to HIV-HBV co-infected groups, to significantly reduce mortality, and contribute to alleviating public health burden.
Keywords
Survival Status, HIV-HBV Co-Infected, HAART, Mekelle City
1. Introduction
The end-stage of liver disease has emerged as the primary cause of death in antiretroviral therapy (ART) patients. HIV and hepatitis B virus (HBV) co-infection are the core causes of episodes of transmissible disease that result from the interruption of ART and the development of HIV-HBV resistance to drug treatment.
| [1] | Chauvel, O., et al., Risk factors for acute liver enzyme abnormalities in HIV-hepatitis B virus-coinfected patients on antiretroviral therapy. Antiviral therapy, 2007. 12(7): p. 1115 CrossRef | Google Scholar. |
[1]
.
Furthermore, there are similarities between the HIV and HBV infection pathways, which typically lead to more severe and progressive liver disease as well as a higher prevalence of hepatocellular carcinoma that progresses more quickly after death. Patients who are co-infected are more likely to require thorough management
| [2] | WHO, Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection: Mar-15. 2015: World Health Organization. |
[2]
, as HIV and HBV remain major global public health issues. are both terminal, and the resistance to antiviral medications typically appears during a phase of treatment that renders HIV-HBV co-infected people clinically ineffective and has complex systemic effects.
| [3] | Kourtis, A. P., et al., HIV–HBV coinfection—A global challenge. New England Journal of Medicine, 2012. 366(19): p. 1749-1752. |
[3]
The HIV-HBV co-infected group has lower rates of hepatitis B surface antigen but higher levels of HBV infection in the blood
| [4] | Tran, T. T., et al., Hepatitis B e antigen status and hepatitis B DNA levels in women of childbearing age with chronic hepatitis B infection screening for clinical trials. PLoS One, 2015. 10(3): p. e0121632. |
[4]
. Individuals co-infected with HIV/HBV have an inferior response to drug therapy, a long-term clinical outcome, a typically burdened risk of liver cirrhosis, and impaired immunological recovery compared to HIV mono-infected patients on ART
| [3] | Kourtis, A. P., et al., HIV–HBV coinfection—A global challenge. New England Journal of Medicine, 2012. 366(19): p. 1749-1752. |
| [5] | Wandeler, G., et al., Hepatitis B virus infection is associated with impaired immunological recovery during antiretroviral therapy in the Swiss HIV cohort study. The Journal of Infectious Diseases, 2013. 208(9): p. 1454-1458. |
[3, 5]
. According to different studies, the developed countries have changes in the main causes of admission, death of HIV patients, and opportunistic diseases progressive to chronic diseases, moreover, neoplasm is associated with other than acquired immune deficiency syndrome (AIDS)
| [6] | Ford, N., et al., Causes of hospital admission among people living with HIV worldwide: a systematic review and meta-analysis. The Lancet HIV, 2015. 2(10): p. e438-e444. |
| [7] | Ingle, S.M., et al., Impact of risk factors for specific causes of death in the first and subsequent years of antiretroviral therapy among HIV-infected patients. Clinical Infectious Diseases, 2014. 59(2): p. 287-297. |
| [8] | Grinsztejn, B., et al., Changing mortality profile among HIV-infected patients in Rio de Janeiro, Brazil: shifting from AIDS to non-AIDS related conditions in the HAART era. PloS one, 2013. 8(4): p. e59768. |
[6-8]
. But, in developing countries, high mortality rates persist despite the availability of ART; AIDS-related events are the main cause of admission and death of clients attending ART
| [9] | Lewden, C., et al., Disease patterns and causes of death of hospitalized HIV‐positive adults in West Africa: a multicountry survey in the antiretroviral treatment era. Journal of the International AIDS Society, 2014. 17(1): p. 18797. |
| [10] | Meintjes, G., et al., HIV-related medical admissions to a South African district hospital remain frequent despite effective antiretroviral therapy scale-up. Medicine, 2015. 94(50). |
[9, 10]
.
Globally, according to the United States Aid International development report, over 38 million people have been living with HIV, and, 690 000 people died from AIDS-related illnesses in 2019. In addition, previously, studies on HBV-related causes of mortality were reviewed among productive young age groups of people between 1990 and 2010 globally and in regional countries
| [11] | Global, H., AIDS statistics–2019 fact sheet (2019). 2020. |
| [12] | Lozano, R., et al., Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 2012. 380(9859): p. 2095-2128. |
[11, 12]
. Moreover, over 26 million people were living with HIV in low- and middle-income countries in 2013
| [13] | WHO., Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: summary of key features and recommendations, June 2013, World Health Organization. |
[13]
.
At the end of 2019, US$ 18.6 billion will be invested for AIDS-related control in low- and middle-income countries around the globe; approximately 57% of the total resources mobilized for HIV/AIDS in developing countries. And the total annual cost per patient of chronic hepatitis B-related diseases was US$ 32958 in 2012
| [11] | Global, H., AIDS statistics–2019 fact sheet (2019). 2020. |
| [14] | Kavosi, Z., et al., Economic burden of hepatitis B virus infection in different stages of disease; a report from southern Iran. Middle East journal of digestive diseases, 2014. 6(3): p. 156. |
[11, 14].
The HBV is a leading cause of liver morbidity and mortality throughout the world, accounting for over 360 million cases of chronic hepatitis and 620,000 deaths annually
| [15] | Musa, B., et al., Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: a systematic review and meta-analysis. Nigerian journal of clinical practice, 2015. 18(2): p. 163-172. |
[15]
. Contradictory reports exist on the role of HBV in HIV disease progression, while some studies have reported no significant effect of HBV on HIV disease progression
| [16] | Thio, C.L., et al., Characterization of HIV-HBV co-infection in a multi-national HIV-infected cohort. AIDS (London, England), 2013. 27(2): p. 191. |
[16]
.
Over 15% of people with HIV in sub-Saharan Africa are living with chronic hepatitis B virus infection
| [17] | Barth, R.E., et al., Hepatitis B/C and HIV in sub-Saharan Africa: an association between highly prevalent infectious diseases. A systematic review and meta-analysis. International Journal of Infectious Diseases, 2010. 14(12): p. e1024-e1031. |
[17]
. Previously studies in the Sub-Saharan African region remains the most burdened, with 24.5 million people affected by HIV, on behalf of a little below two-thirds of all people living with HIV around the globe
| [18] | Oladeinde, B.H., et al., Prevalence of HIV and anemia among pregnant women. North American journal of medical sciences, 2011. 3(12): p. 548. |
[18]
. In the previous analysis in 2012, approximately 1.2 million people died from HIV-related causes in the African region
. Other studies that have been reported in Sub–Saharan Africa remain the most affected region, with 24.5 million people living with HIV
| [18] | Oladeinde, B.H., et al., Prevalence of HIV and anemia among pregnant women. North American journal of medical sciences, 2011. 3(12): p. 548. |
[18]
.
In Ethiopia, there are some studies regarding the prevalence of HBV among HIV patients, in the north-west Gondar, it showed 5.6%
| [20] | Wondimeneh, Y., et al., HBV and HCV seroprevalence and their correlation with CD4 cells and liver enzymes among HIV positive individuals at the University of Gondar Teaching Hospital, Northwest Ethiopia. Virology journal, 2013. 10(1): p. 171. |
[20]
, and other studies in Mekelle Hospital have been 5.9%
| [21] | Weldmart, L., et al., Sero-prevalence of HBV and associated risk factors among HIV positive individuals attending ART clinic at Mekelle hospital, Tigray, Northern Ethiopia. AIDS research and therapy, 2016. 13(1): p. 6. |
[21]
. This research topic may be useful for managing patients undergoing antiretroviral therapy (ART), as well as for providing social support to co-infected individuals with HIV and HIV patients residing in ART clinics. Furthermore, the HIV care package in Ethiopia omitted to include the hepatitis B virus when gathering baseline data for subsequent cohort-related research. The purpose of this study was to compare the survival status of HIV-HBV co-infection with HIV mono-infected patients on highly antiretroviral therapy (HAART) in Mekelle City, North Ethiopia.
2. Methods
2.1. Study Design and Settings
An institutional-based retrospective cohort study was conducted from March 1-30, 2018, in Mekelle City, Tigray, Ethiopia. Mekelle is the capital city of Tigray regional state, located in the northern part of Ethiopia, at 783 km from the capital city of Addis Ababa. The city is administratively divided into 7 sub-cities. The city has one referral hospital, 2 general hospitals, 9 health centers, and 48 private clinics
| [22] | Deter, B. M., minants of Demand for Health Care Services in Mekelle City. 2013. |
[22]
. Among these, 14 health facilities (HFs) provide ART services for over 12,277 patients taking ART by 2018. According to the projected central statistical agency of Ethiopia in 2018, a total population of 340,859 people resides in the city.
2.2. Source and Study Population
The HIV-infected patients under ART registered in Mekelle Health facilities were considered the source population, and all registered adult patients who had started ART with positive HBV (exposed group) and HBV negative (unexposed group) in selected 6HFs were also the study population. In addition, a known HBV status who started ART on the registered patient card in these 6HFs were also the study subjects.
2.3. Eligibility Criteria
All registered patients greater than or equal to 15 years old, whoever started ART with known HBV status from January 2009 to February 2018, were an inclusion criterion, whereas, incomplete patient cards, unknown HBV results, and children <15 years old were considered an exclusion criterion of the study.
2.4. Sample Size and Sampling Procedures
The sample size determined was calculated using Epi-Info statistical package 7, exposed and unexposed subjects with the assumption of two-sided confidence limits = 95%, pow r =80 %, the ratio of (unexposed: exposed group) = 4:1, and the percent of outcome in the unexposed group (mortality of HIV mono-infected group) = 5.3%
| [23] | Mbae M., et alEarly mortality risk of HIV/Hepatitis B Virus co-infected patients initiating in Kenya. WWW.Lshtm,ac.uk 2015. |
[23]
. Risk ratio (HIV-HBV co-infected) = 3.32
| [23] | Mbae M., et alEarly mortality risk of HIV/Hepatitis B Virus co-infected patients initiating in Kenya. WWW.Lshtm,ac.uk 2015. |
[23]
. Percent outcome in the exposed group = 17.6%. To this end, the total number of study participants was 233 patients, of which 47 were exposed and 186 were unexposed. The systematic random sampling method was used, and sampling technique or procedure among the total number of 14 ART health facilities. By using a simple random sampling method, six health facilities were selected with a total of 6515 clients who had ever started ART in the previous years of registered data, using the systematic random sampling method, and the sample size was double increased using the design effect (233*2 = 466; of which 94 were exposed and 372 were unexposed). The proportional sample allocation is done for each 6HF; additionally, patient cards are reviewed every 24 intervals (N/n 6515/466). Verbal consent done from a live patient card and written informed consent applied for children 15-18 years old.
2.5. Study Variables
The dependent variable was time-to-death, and the independent variables, HBV status: Hepatitis B virus-positive and negative results in ART patients, and the other variables like
The socio-demographic characteristics: sex, age, marital status, occupation, educational status, and the clinical and laboratory characteristics: Baseline CD4 cell count, baseline hemoglobin level, tuberculosis, baseline nutritional status (BMI), baseline ALT level, baseline AST Level, baseline creatinine, and baseline WHO clinical stage.
2.6. Operational Definitions
Survival: when the patient is known to be alive as evidenced by his/her clinical follow-up till the end of the study period.
Time-to-death: The time from entry into a study on ART until a subject has a particular outcome (death) during the follow-up period (time entry from January 2009 to February 2018 and the time follow-up evaluated in March 2018).
Incomplete card: when two or more of the independent variables are not recorded in the patient registration card.
Censored: Observations of event histories and occurs when the information about duration is incomplete.
Right censoring: proportion of the individuals studied, we have not observed them until death, but only up to some point in time (where they were still alive).
1. Drop out: patients known to have stopped ART for more than three months’ duration for any reason.
2. Lost to follow-up: patients who missed visits to the same health facilities until 3 months after the last scheduled.
3. Transfer out: Individuals initiated ART in the health facility and formally transferred to another health facility.
Death: the patient was recorded as dead on the exit patient individual registration chart.
2.7. Data Collection Tools and Data Management
Data were collected using a data extraction format (checklist) from different journals and medical records of HIV patients
| [23] | Mbae M., et alEarly mortality risk of HIV/Hepatitis B Virus co-infected patients initiating in Kenya. WWW.Lshtm,ac.uk 2015. |
| [24] | Griensven J., Phirum L., ChounK., ThaiK., Weggheleire., Lynen L., Hepatitis B and C Co-Infection among HIV-Infected Adults while on Antiretroviral Treatment: Long-Term Survival, CD4 Cell Count Recovery and Antiretroviral Toxicity in Cambodia. PLOS ONE, 2014. 9(2): p. 3-4. |
| [25] | Sarkar J., Saha D., Bandyopadhyay B. et al., Baseline characteristics of HIV & hepatitis B virus (HIV/HBV) co-infected patients from Kolkata, India. Indian J Med Res 2016. |
[23-25]
. The data collection process also involved using the unique medical record number of eligible groups extracted from the ART registration logbook, and then based on the unique medical record number; the chart of the patient was retrieved from the medical record room. We started data collection time from the date of ART initiated and serological tested for hepatitis B virus, and patient cards were followed until time to event. The status of the clients was reviewed by trained BSc nurses and laboratory technologists who are experienced on ART.
To ensure data quality, training was provided for one supervisor and four data collectors. The pretest was conducted on 5% of the sample size in Mekelle HFs using selected medical charts of the eligible patients who were registered in the ART registration logbook. Double data entry was used to minimize errors. In addition to this, close supervision of data collectors by the supervisor was continued during the data collection period.
2.8. Data Processing and Statistical Analysis
Data were coded, cleaned, checked, and entered in Epi Info version 7. Export data to Stata version 14 for analysis.
Kaplan Meier was applied to estimate the probability of survival trend and median time to death divided by person-years observation (PYO) of follow-up with a 95% confidence interval (CI) after ART initiation of known Hepatitis B virus status for two groups.
A log-rank test was used to compare the median time to death between the two groups on ART using Kaplan-Meier survival curves, with the null hypothesis being tested that there is no difference in the distribution of the survival curves. The graph is not a straight line, indicating that a Cox regression method was applied in this survival analysis for survival time.
Model building strategy: The 1st step was a bivariate analysis to show the relationship between survival time and each important covariate; variables were imported to the multivariate with a p-value <0.25. Then the cox regression in the multivariate model was fitted to all variables using the forward elimination technique to assess confounders, moreover, it was assessed by purposeful selection of variables greater or equal to 10%. Collinearity was evaluated by calculating the variance inflation factors. Additionally, an interaction was checked by each significant variable with an insignificant variable in multivariate analysis, and finally a variable with Wald p-values less than 0.05 had been declared in the final model.
Assessment of model fitness: The assumption of the proportional hazards model was checked by a scaled Schoenfeld residual of a global test conducted for testing the assumption of cox proportional hazard. The goodness of fit of the final model was checked by using the Cox-Snell residuals.
3. Results
3.1. Survival Analyses in HIV-HBV Co-Infected with HIV Mono-Infected Groups
Socio-demographic characteristics: All the study cohorts initiated treatment between January 2009 and February 2018, and a total of 6515 patients were registered in the study unit; among these, a total of 466 patient cards were evaluated, of which 94 HIV-HBV co-infected (exposed) and 372 HIV mono-infected (unexposed) groups were identified.
Out of the total cases, 300 (64.3%) were females, and the median age of the HBV-exposed group was 35, ranging from 15 to 65 years. On the other hand, the median age of the HBV- unexposed group was 33 (ranging from 15 to 68). Among the total cases in the HBV exposed group, 42 (44.7%) were married, 21 (22.3%) never married, 20 (21.3%) divorced, and 11 (11.7%) widowed. While from those HBV unexposed groups, 174 (46.8%) were married, 87 (23.4%) never married, 79 (21.2%) divorced, and 32 (8.6%) were widowed.
Clinical and laboratory characteristics: cluster of differentiation4 cell count (CD4), among the HBV-exposed group greater than 200 cells/µl was 36 (38.3%) and less than or equal to 200 cells count 58 (61.7%) cases were evaluated. On the other hand, the CD4 cell count in the HBV unexposed group on >200 cell/µl was 219 (58.9) and <200 cell/µl 153 (41.1%).
Fifty-seven (56.4%) had normal (0-40 unit) Alanine Aminotransferase (ALT) levels, and 41 (43.6%) had abnormal ALT levels in the HBV-exposed group, whereas in the unexposed HBV group, 311 (83.5) cases had normal ALT levels and 61 (16.4%) cases had abnormal ALT levels
| [26] | WHO, Training workshop on screening, diagnosis and treatment of hepatitis B and C. |
[26]
.
3.2. Comparison of HIV-HBV Co-Infected with HIV Mono-Infected Groups on Survival Time
During the follow-up period, 49 (10.5%) patients died in both groups, of which 23 (24.4%) were co-infected and 26 (6.99%) were HIV mono-infected groups. Among the total censored, four patients were in the HBV exposed group, and six patients were also in the HBV unexposed group (
Table 1).
Table 1. Outcome of HIV-HBV co-infected and HIV mono infected adult patients on survival time attending ART in Mekelle city, Tigray, Ethiopia, from January 2009 to February 2018.
Variables | Category | Both groups | Exposed=94(20%) | Unexposed=372(80%) |
No (%) | No (%) | No (%) |
Follow-up outcome | Lost to follow up | 11(2.36) | 2(2.13) | 9(2.42) |
Drop out | 10(2.15) | 4(4.26) | 6(1.61) |
Transfer out | 10(2.15) | 1(1.06) | 9(2.42) |
Alive | 386(82.8) | 64(68.09) | 322(86.56) |
Death (events) | 49(10.5) | 23(24.47) | 26(6.99) |
3.3. Median Survival Time and Mortality Rate
The median survival time of HIV-HBV co-infected patients on ART was 8.45 years with a total 401-person year observation (PYO) time at risk, but we couldn’t calculate for mono-infected patients due to commutative survival time greater than 81% of patients were censored. And the crude hazard rate of mortality among HIV-HBV co-infected and HIV mono-infected patients initiating ART were 5.73 and 1.67 per 100-person year’s observation, respectively (
Table 2).
Table 2. Outcome of mortality rate among HIV-HBV co-infected and HIV mono-infected patients attending ART in Mekelle city, from January 2009 to February 2018.
Infection status | Number of deaths | Total PYs of Follow-up Time at Risk | Mortality rate (per 100 PYs, 95% CI) |
HIV mono-infected | 26 | 1559 | 1.67 (1.13-2.44) |
HIV/HBV co-infected | 23 | 401 | 5.73 (3.81-8.62) |
Total | 49 | 1960 | 2.49(1.89-8.63) |
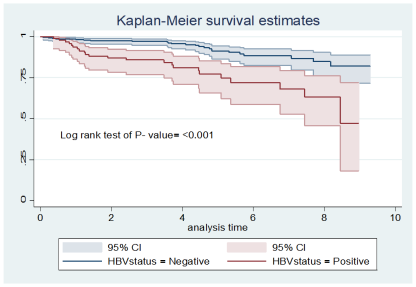
3.4. Survival Estimation by Kaplan-Meier curve
The cumulative survival probability in the categories of HIV-HBV co-infected and HIV mono-infected patients in both groups was statistically significant by the log-rank test of P<0.001. Survival estimation focused on HBV serological interesting showed that HIV-HBV co-infected individuals had the poorest survival compared to HIV mono-infected clients (
Figure 1).
Figure 1. Kaplan Meier survival estimation in time-years follows up on HIV-HBV co-infected and HIV mono-infected groups in Mekelle city from January 2009 to February 2018.
3.5. Survival Analysis Using the Cox Regression Model
In the final process of backward elimination on multivariable cox regression analysis, HBV co-infected (adjusted HR 2.35, 95% CI 1.31-4.21). WHO stage (adjusted HR 2.36, 95% CI 1.13-4.95, and Tuberculosis (Adjusted HR 2.70, 95% CI 1.48-4.90) were statistically significant over time between two groups (
Table 3).
Table 3. Outcome of HIV-HBV co-infection on mortality change in periods after ART initiation in Mekelle city, from January 2009 to February 2018.
_t | |Hazard Ratio | Std, Err | Z | P>|z| | [95%Conf. Interval] |
HBV status | | | | | |
Negative | 1 | | | | Reference |
Positive | 2.35796 | .698 | 2.89 | 0.004 | 1.318-4.214 |
WHO Stage | | | | | |
Stages I and II | 1 | | | | Reference |
Stages II and IV | 2.365 | .891 | 2.29 | 0.022 | 1.130-4.951 |
Tuberculosis | | | | | |
No | 1 | | | | Reference |
Yes | 2.702 | .822 | 3.27 | 0.001 | 1.489-4.905 |
Key: HBV-Hepatitis B virus, WHO-World Health Organization, TB-Tuberculosis, ART-Antiretroviral Therapy
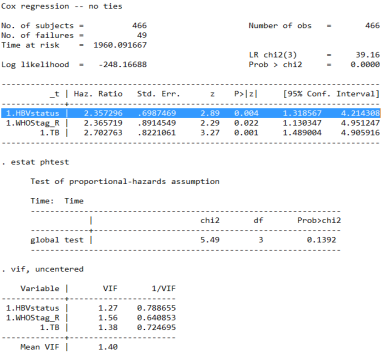
During the backward elimination process of Cox regression model analysis, there was no interaction between variables, but hemoglobin was found to be a potential confounder. The statistical test was used to assess the proportional hazard assumption, and the global test, which was based on the scaled Schoenfeld residuals, did not suggest a violation of the proportional hazard assumption for all covariates (probability of Chi-square>0.05). Finally, multicollinearity was also assessed using a variance inflation factor (VIF) that was 1.40 (Appendix 1).
4. Discussion
The median age of the HBV exposed group was 35 (range 15 to 65), and the median age for the HBV unexposed group was 33, range 15 to 68. During the follow-up period, 49 (10.5%) patients died from both groups, of which 23 (24.4%) were HIV-HBV co-infected and 26 (6.99%) were HIV mono-infected groups. And the crude hazard rate of mortality among HIV-HBV co-infected was 5.73, and in the HIV mono-infected patients in ART was 1.67 per 100-person year’s observation. In multivariable Cox regression analysis, HBV status, WHO stage, and tuberculosis were potential risk factors for the survival of HIV patients.
In our study, over the 1960-person-year observation risk time, the hazard rate of mortality on HIV-HBV co-infected and HIV mono-infected patients initiating ART were 5.73 and 1.67 per 100 person-years, respectively. This result is that the influence of HBV co-infection on the mortality of HIV patients is a controversial issue in most studies, such as Euro-SIDA. Similar significantly higher mortality for HBV co-infected patients as compared with HIV patients was 3.7 versus 2.6 per 100 person-years, and in another study, mortality was 0.7 versus. 0.2 per 100 person-years observation
| [27] | Sheng WH, C. M., Hsieh SM, Hsiao CF, Wang JT, Hung CC, et al., Impact of chronic hepatitis B virus (HBV) infection on outcomes of patients infected with HIV in an area where HBV infection is hyperendemic. Clin Infect Dis, 2004. 38: p. 1471-7. |
[27]
. Similarly, a cohort study from Denmark also found a significantly higher mortality rate for Hepatitis B surface antigen positive individuals compared to Hepatitis B surface antigen negative patients on HIV commencement ART was 3.9 and 2.5 per 100 person-years, respectively
| [28] | al, O. K. e., Hepatitis B prevalence and influence on HIV treatment outcome and mortality in the Chilean AIDS Cohort, International Journal of Infectious Diseases, 2013: p. 920. |
[28]
.
The result of cox regression multivariate analysis in the present study, the mortality rate of HIV-HBV co-infection was higher significant than HIV mono-infection patient’s survival on ART, at HR 2.35 (95% CI 1.31-4.21), and the study is in line with the study conducted in Chilean AIDS cohort analysis, United States of America, and Thailand
| [28] | al, O. K. e., Hepatitis B prevalence and influence on HIV treatment outcome and mortality in the Chilean AIDS Cohort, International Journal of Infectious Diseases, 2013: p. 920. |
| [29] | Chun, H. M., et al., HIV outcomes in Hepatitis B virus coinfected individuals on HAART. Journal of acquired immune deficiency syndromes (1999), 2014. 66(2): p. 197-205. |
| [30] | Tsuchiya, N., et al., Chronic hepatitis B and C co-infection increased all-cause mortality in HAART-naive HIV patients in northern Thailand. Epidemiology & Infection, 2013. 141(9): p. 1840-1848. |
[28-30]
.
This higher mortality in HBV co-infection was mostly due to liver-related mortality as per studies in Euro-SIDE
| [27] | Sheng WH, C. M., Hsieh SM, Hsiao CF, Wang JT, Hung CC, et al., Impact of chronic hepatitis B virus (HBV) infection on outcomes of patients infected with HIV in an area where HBV infection is hyperendemic. Clin Infect Dis, 2004. 38: p. 1471-7. |
[27]
, and hepatitis-related co-infection mortality was the most common cause of death in Chinese
| [31] | al., Y.e., Impact of hepatitis B virus infection on HIV response to antiretroviral therapy in a Chinese antiretroviral therapy center, International Journal of Infectious Diseases 28 (2014) 31, 2014. 28 p. 31. |
[31]
. However, the discrepancy of higher death in hepatitis co-infection was not known and not diagnosed with liver-related mortality, studied in Thailand at Lampang Hospital
| [30] | Tsuchiya, N., et al., Chronic hepatitis B and C co-infection increased all-cause mortality in HAART-naive HIV patients in northern Thailand. Epidemiology & Infection, 2013. 141(9): p. 1840-1848. |
[30]
.
In our study, it was found that the hazard of mortality after ART started was a 2.3-fold higher risk of mortality in the HIV-HBV co-infected group, this result is similar to the study conducted on developing countries in Cambodia, Nigeria, Ghana, and Kenya compared to the HIV mono-infected group
| [32] | Sarfo, F.S., et al., Long-term responses to first-line antiretroviral therapy in HIV and hepatitis B co-infection in Ghana. Journal of Infection, 2014. 69(5): p. 481-489. |
| [33] | van Griensven., et al., Hepatitis B and C co-infection among HIV-infected adults while on antiretroviral treatment: long-term survival, CD4 cell count recovery and antiretroviral toxicity in Cambodia. PloS one, 2014. 9(2): p. e88552. |
| [34] | Tathiah, N., HIV, and hepatitis B/C co-infection in KwaZulu-Natal from 2002 to 2010: a retrospective database analysis. 2015. |
[32-34]
. This possible explanation may be due to the similar setup on the burden of HIV-HBV co-infection occurring in most resource-limited countries
| [35] | Di Bisceglie., et al., HIV–HBV coinfection among South African patients receiving antiretroviral therapy. Antiviral therapy, 2010. 15(3 Pt B): p. 499. |
[35]
.
Strength and limitation: A longitudinal cohort study was a higher opportunity to screen patients on hepatitis B surface antigen status and start antiretroviral therapy.The limitation of our study was that Hepatitis testing was not performed for all patients in the Mekelle health facilities as part of the routine test for patients initiating ART. Therefore, the quality of data obtained from these findings was highly dependent on the completeness of patient cards, typically HBV screen status, and other variables. And, we couldn’t get patient cards based on K-interval due to most patient cards unknown HBV status, which may lead to sample selection bias.
5. Conclusion and Recommendations
In conclusion, our study revealed that the multivariate proportional hazards cox regression model of higher risk of death was evaluated in HBV-HIV co-infected patients attending ART. Hepatitis B status, WHO clinical stage, and tuberculosis are potential risk factors for the change in the survival time of patients on antiretroviral treatment, and also HIV mono-infected patients have better survival time than HIV-HBV co-infected patients during the 1960-person-year assessment. And recommend to Mekelle health facilities that special attention is given to patients on HIV-positive ART with HBV-co-infected individuals for progressive survival time. And a prospective cohort will be recomended.
Abbreviations
AIDS | Acquired Immune Deficiency Syndrome |
AHR | Adjusted Hazard Ratio |
ALT | Alanine Transaminase |
HART | Highly Antiretroviral Therapy |
AST | Aspartate Transaminase |
CD4 | Cluster of Differentiation Receptor 4 |
CHR | Crude Hazard Ratio |
DNA | Deoxyribonucleic Acid |
HBsAg | Hepatitis B Surface Antigen |
HBV | Hepatitis B Virus |
HIV | Human Immunodeficiency Virus |
HR | Hazard Ratio |
IQR | Interquartile |
SD | Standard Deviation |
TB | Tuberculosis |
TPO | Time Person Observation |
WHO | World Health Organization |
Acknowledgments
We would like to express our gratitude to Mekelle University, the college of health science, the department of epidemiology, and the Tigray regional health bureau for providing this golden opportunity. Special thanks to Sr. Mulu Fitum, Sr. Hadas Brhanu, and Mr. Gebrebrhan Brhane for those who have participated in the data collection and in the research process.
Authors Contributions
Haileselassie Bisrat Bidre: Conceptualization, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review & editing
Desalegn Massa Teklemicael: Conceptualization, Formal Analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing
Goshu Hagos Gebrewahid: Methodology, Supervision, Visualization, Writing – review & editing
Gebrecherkos Teame: Methodology, Supervision, Visualization, Writing – review & editing
Fsaha Gebretsadkan Tekulu: Methodology, Supervision, Visualization, Writing – review & editing
Alemayehu Bayray Kahsay: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing
Ethical Approval and Informed Consent
The ethical approval of the research was made by the Mekelle University College of Health Sciences-Ethical Review Committee (ERC-1350/2018). As a retrospective study, this study was conducted on already available data that were collected during routine clinical practices. The dataset used for analysis was kept anonymously and used for the intended research only. Accordingly, the research ethics review committee determined that a written informed consent from each patient was unnecessary. Instead, permission to use the information in the database for the purposes of the research was obtained from the regional health bureau and the health facilities that own the dataset. All the methods of this study were performed in accordance with the ethical evaluation of the Helsinki Declaration of Human Research.
Funding
No external funding
Data Availability Statement
The data set of this study is available from the corresponding author upon reasonable request.
Conflicts of Interest
The author declares no conflicts of interest.
Appendix
Annexes: Steps of confounder assessment in back ward cox regression model
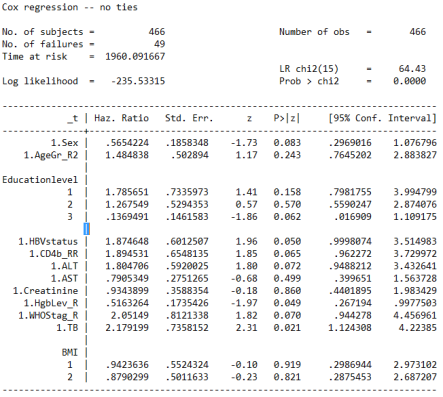
Step One
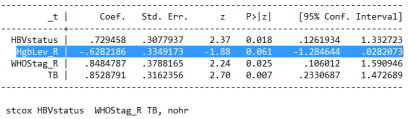
Figure 2. During the backward elimination procedure of the Cox regression model analysis, identification of confounding factor and interactions.
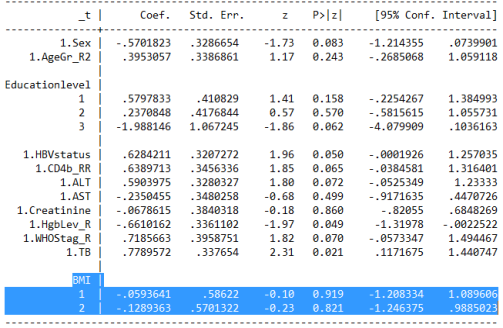
Step Two
Figure 3. During the backward elimination procedure of the Cox regression model analysis, Body Mass Index (BMI) was identified as a possible confounding factor, but no interactions.
Step Three
Figure 4. During the backward elimination procedure of the Cox regression model analysis, Aspartate trans amainase (AST) was identified as a possible confounding factor, but no interactions.
Step Four
Figure 5. During the backward elimination procedure of the Cox regression model analysis, cretinine was identified as a possible confounding factor, but no interactions.
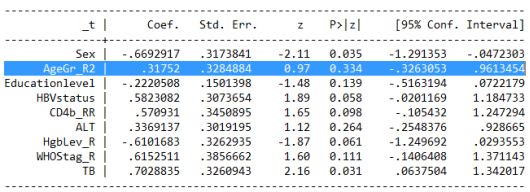
Step Five
Figure 6. During the backward elimination procedure of the Cox regression model analysis, age group was identified as a possible confounding factor, but no interactions.
Step Six
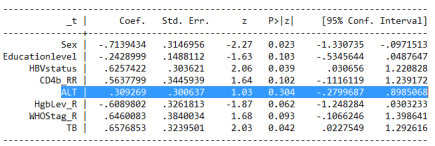
Figure 7. During the backward elimination procedure of the Cox regression model analysis, Alanine Trans aminase (ALT) was identified as a possible confounding factor, but no interactions.
Step Seven
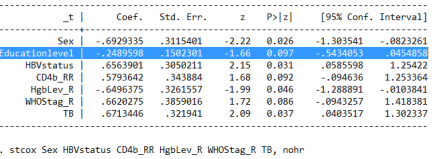
Figure 8. During the backward elimination procedure of the Cox regression model analysis, educational level was identified as a possible confounding factor, but no interactions.
Step Eight
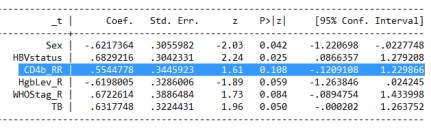
Figure 9. During the backward elimination procedure of the Cox regression model analysis, CD4 was identified as a possible confounding factor, but no interactions.
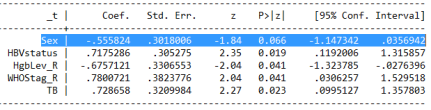
Figure 10. During the backward elimination procedure of the Cox regression model analysis, sex was identified as a possible confounding factor, but no interactions.
Figure 11. During the backward elimination procedure of the Cox regression model analysis, hemoglobin level was identified as a possible confounding factor, but no interactions.
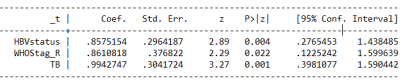
Figure 12. During the final back ward élimination procès of the Cox régression model analyses, there was no possible confounding factor and interactions.
Figure 13. Final statically significant in cox regression, checked by global test and Variance inflation factor (VIF).
References
| [1] |
Chauvel, O., et al., Risk factors for acute liver enzyme abnormalities in HIV-hepatitis B virus-coinfected patients on antiretroviral therapy. Antiviral therapy, 2007. 12(7): p. 1115 CrossRef | Google Scholar.
|
| [2] |
WHO, Guidelines for the prevention, care and treatment of persons with chronic hepatitis B infection: Mar-15. 2015: World Health Organization.
|
| [3] |
Kourtis, A. P., et al., HIV–HBV coinfection—A global challenge. New England Journal of Medicine, 2012. 366(19): p. 1749-1752.
|
| [4] |
Tran, T. T., et al., Hepatitis B e antigen status and hepatitis B DNA levels in women of childbearing age with chronic hepatitis B infection screening for clinical trials. PLoS One, 2015. 10(3): p. e0121632.
|
| [5] |
Wandeler, G., et al., Hepatitis B virus infection is associated with impaired immunological recovery during antiretroviral therapy in the Swiss HIV cohort study. The Journal of Infectious Diseases, 2013. 208(9): p. 1454-1458.
|
| [6] |
Ford, N., et al., Causes of hospital admission among people living with HIV worldwide: a systematic review and meta-analysis. The Lancet HIV, 2015. 2(10): p. e438-e444.
|
| [7] |
Ingle, S.M., et al., Impact of risk factors for specific causes of death in the first and subsequent years of antiretroviral therapy among HIV-infected patients. Clinical Infectious Diseases, 2014. 59(2): p. 287-297.
|
| [8] |
Grinsztejn, B., et al., Changing mortality profile among HIV-infected patients in Rio de Janeiro, Brazil: shifting from AIDS to non-AIDS related conditions in the HAART era. PloS one, 2013. 8(4): p. e59768.
|
| [9] |
Lewden, C., et al., Disease patterns and causes of death of hospitalized HIV‐positive adults in West Africa: a multicountry survey in the antiretroviral treatment era. Journal of the International AIDS Society, 2014. 17(1): p. 18797.
|
| [10] |
Meintjes, G., et al., HIV-related medical admissions to a South African district hospital remain frequent despite effective antiretroviral therapy scale-up. Medicine, 2015. 94(50).
|
| [11] |
Global, H., AIDS statistics–2019 fact sheet (2019). 2020.
|
| [12] |
Lozano, R., et al., Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 2012. 380(9859): p. 2095-2128.
|
| [13] |
WHO., Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: summary of key features and recommendations, June 2013, World Health Organization.
|
| [14] |
Kavosi, Z., et al., Economic burden of hepatitis B virus infection in different stages of disease; a report from southern Iran. Middle East journal of digestive diseases, 2014. 6(3): p. 156.
|
| [15] |
Musa, B., et al., Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: a systematic review and meta-analysis. Nigerian journal of clinical practice, 2015. 18(2): p. 163-172.
|
| [16] |
Thio, C.L., et al., Characterization of HIV-HBV co-infection in a multi-national HIV-infected cohort. AIDS (London, England), 2013. 27(2): p. 191.
|
| [17] |
Barth, R.E., et al., Hepatitis B/C and HIV in sub-Saharan Africa: an association between highly prevalent infectious diseases. A systematic review and meta-analysis. International Journal of Infectious Diseases, 2010. 14(12): p. e1024-e1031.
|
| [18] |
Oladeinde, B.H., et al., Prevalence of HIV and anemia among pregnant women. North American journal of medical sciences, 2011. 3(12): p. 548.
|
| [19] |
The global health sector strategy on HIV/AIDS 2011-2015: an interim review of progress: abridged report, May 2014.
https://iris.who.int/handle/10665/112790
|
| [20] |
Wondimeneh, Y., et al., HBV and HCV seroprevalence and their correlation with CD4 cells and liver enzymes among HIV positive individuals at the University of Gondar Teaching Hospital, Northwest Ethiopia. Virology journal, 2013. 10(1): p. 171.
|
| [21] |
Weldmart, L., et al., Sero-prevalence of HBV and associated risk factors among HIV positive individuals attending ART clinic at Mekelle hospital, Tigray, Northern Ethiopia. AIDS research and therapy, 2016. 13(1): p. 6.
|
| [22] |
Deter, B. M., minants of Demand for Health Care Services in Mekelle City. 2013.
|
| [23] |
Mbae M., et alEarly mortality risk of HIV/Hepatitis B Virus co-infected patients initiating in Kenya.
WWW.Lshtm,ac.uk
2015.
|
| [24] |
Griensven J., Phirum L., ChounK., ThaiK., Weggheleire., Lynen L., Hepatitis B and C Co-Infection among HIV-Infected Adults while on Antiretroviral Treatment: Long-Term Survival, CD4 Cell Count Recovery and Antiretroviral Toxicity in Cambodia. PLOS ONE, 2014. 9(2): p. 3-4.
|
| [25] |
Sarkar J., Saha D., Bandyopadhyay B. et al., Baseline characteristics of HIV & hepatitis B virus (HIV/HBV) co-infected patients from Kolkata, India. Indian J Med Res 2016.
|
| [26] |
WHO, Training workshop on screening, diagnosis and treatment of hepatitis B and C.
|
| [27] |
Sheng WH, C. M., Hsieh SM, Hsiao CF, Wang JT, Hung CC, et al., Impact of chronic hepatitis B virus (HBV) infection on outcomes of patients infected with HIV in an area where HBV infection is hyperendemic. Clin Infect Dis, 2004. 38: p. 1471-7.
|
| [28] |
al, O. K. e., Hepatitis B prevalence and influence on HIV treatment outcome and mortality in the Chilean AIDS Cohort, International Journal of Infectious Diseases, 2013: p. 920.
|
| [29] |
Chun, H. M., et al., HIV outcomes in Hepatitis B virus coinfected individuals on HAART. Journal of acquired immune deficiency syndromes (1999), 2014. 66(2): p. 197-205.
|
| [30] |
Tsuchiya, N., et al., Chronic hepatitis B and C co-infection increased all-cause mortality in HAART-naive HIV patients in northern Thailand. Epidemiology & Infection, 2013. 141(9): p. 1840-1848.
|
| [31] |
al., Y.e., Impact of hepatitis B virus infection on HIV response to antiretroviral therapy in a Chinese antiretroviral therapy center, International Journal of Infectious Diseases 28 (2014) 31, 2014. 28 p. 31.
|
| [32] |
Sarfo, F.S., et al., Long-term responses to first-line antiretroviral therapy in HIV and hepatitis B co-infection in Ghana. Journal of Infection, 2014. 69(5): p. 481-489.
|
| [33] |
van Griensven., et al., Hepatitis B and C co-infection among HIV-infected adults while on antiretroviral treatment: long-term survival, CD4 cell count recovery and antiretroviral toxicity in Cambodia. PloS one, 2014. 9(2): p. e88552.
|
| [34] |
Tathiah, N., HIV, and hepatitis B/C co-infection in KwaZulu-Natal from 2002 to 2010: a retrospective database analysis. 2015.
|
| [35] |
Di Bisceglie., et al., HIV–HBV coinfection among South African patients receiving antiretroviral therapy. Antiviral therapy, 2010. 15(3 Pt B): p. 499.
|
Cite This Article
-
APA Style
Bidre, H. B., Teklemicael, D. M., Gebrewahid, G. H., Teame, G., Tekulu, F. G., et al. (2025). Survival Status of HIV-Hepatitis B Virus Co-Infection with HIV Mono-infected Patients on Antiretroviral Therapy in Mekelle City, North Ethiopia: A Retrospective Cohort Study. International Journal of HIV/AIDS Prevention, Education and Behavioural Science, 11(1), 18-29. https://doi.org/10.11648/j.ijhpebs.20251101.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Bidre, H. B.; Teklemicael, D. M.; Gebrewahid, G. H.; Teame, G.; Tekulu, F. G., et al. Survival Status of HIV-Hepatitis B Virus Co-Infection with HIV Mono-infected Patients on Antiretroviral Therapy in Mekelle City, North Ethiopia: A Retrospective Cohort Study. Int. J. HIV/AIDS Prev. Educ. Behav. Sci. 2025, 11(1), 18-29. doi: 10.11648/j.ijhpebs.20251101.13
Copy
|
Download
AMA Style
Bidre HB, Teklemicael DM, Gebrewahid GH, Teame G, Tekulu FG, et al. Survival Status of HIV-Hepatitis B Virus Co-Infection with HIV Mono-infected Patients on Antiretroviral Therapy in Mekelle City, North Ethiopia: A Retrospective Cohort Study. Int J HIV/AIDS Prev Educ Behav Sci. 2025;11(1):18-29. doi: 10.11648/j.ijhpebs.20251101.13
Copy
|
Download
-
@article{10.11648/j.ijhpebs.20251101.13,
author = {Haileselassie Bisrat Bidre and Desalegn Massa Teklemicael and Goshu Hagos Gebrewahid and Gebrecherkos Teame and Fsaha Gebretsadkan Tekulu and Alemayehu Bayray Kahsay},
title = {Survival Status of HIV-Hepatitis B Virus Co-Infection with HIV Mono-infected Patients on Antiretroviral Therapy in Mekelle City, North Ethiopia: A Retrospective Cohort Study
},
journal = {International Journal of HIV/AIDS Prevention, Education and Behavioural Science},
volume = {11},
number = {1},
pages = {18-29},
doi = {10.11648/j.ijhpebs.20251101.13},
url = {https://doi.org/10.11648/j.ijhpebs.20251101.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijhpebs.20251101.13},
abstract = {Background: HIV/AIDS and hepatitis B virus (HBV) are two serious global health threats that co-occur and are resistant to antiretroviral therapy (ART). Milions of people worldwide lost their lives to acquired immunodeficiency in 2019.Thus, this study was aimed to evaluate the survival status of patients co-infected with HIV and hepatitis B viruses who are on antiretroviral therapy (HART). Methods: A retrospective cohort study design was conducted. Individuals with HIV-HBV co-infected with HIV mono-infected in six health facilities in Mekelle City from January 2009 to February 2018. The total sample size was 466, of which 94 were HBV exposed and 372 were unexposed for HBV on ART clients. Kaplan-Meier survival and Cox proportional hazard models for survival analysis were used. Data was analyzed using STATA version 14. Result: Of the total patients, 300 (64.3%) were females and most age groups were 15-30 years old, 199 (43%). Over 1960 person years of observation time at risk, 23 (24%) HIV-HBV co-infected and 26 (7%) HIV mono-infected died. In the adjusted analysis, HIV-HBV co-infected group had a 2.53 times increased hazard of death (aHR: 2.52; 95% CI: 1.31-4.85) than HIV mono-infected. Conclusion: In this cohort study, mortality is higher in the HIV-HBV co-infected group. Hence, special attention shall be given to HIV-HBV co-infected groups, to significantly reduce mortality, and contribute to alleviating public health burden.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Survival Status of HIV-Hepatitis B Virus Co-Infection with HIV Mono-infected Patients on Antiretroviral Therapy in Mekelle City, North Ethiopia: A Retrospective Cohort Study
AU - Haileselassie Bisrat Bidre
AU - Desalegn Massa Teklemicael
AU - Goshu Hagos Gebrewahid
AU - Gebrecherkos Teame
AU - Fsaha Gebretsadkan Tekulu
AU - Alemayehu Bayray Kahsay
Y1 - 2025/01/23
PY - 2025
N1 - https://doi.org/10.11648/j.ijhpebs.20251101.13
DO - 10.11648/j.ijhpebs.20251101.13
T2 - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JF - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
JO - International Journal of HIV/AIDS Prevention, Education and Behavioural Science
SP - 18
EP - 29
PB - Science Publishing Group
SN - 2575-5765
UR - https://doi.org/10.11648/j.ijhpebs.20251101.13
AB - Background: HIV/AIDS and hepatitis B virus (HBV) are two serious global health threats that co-occur and are resistant to antiretroviral therapy (ART). Milions of people worldwide lost their lives to acquired immunodeficiency in 2019.Thus, this study was aimed to evaluate the survival status of patients co-infected with HIV and hepatitis B viruses who are on antiretroviral therapy (HART). Methods: A retrospective cohort study design was conducted. Individuals with HIV-HBV co-infected with HIV mono-infected in six health facilities in Mekelle City from January 2009 to February 2018. The total sample size was 466, of which 94 were HBV exposed and 372 were unexposed for HBV on ART clients. Kaplan-Meier survival and Cox proportional hazard models for survival analysis were used. Data was analyzed using STATA version 14. Result: Of the total patients, 300 (64.3%) were females and most age groups were 15-30 years old, 199 (43%). Over 1960 person years of observation time at risk, 23 (24%) HIV-HBV co-infected and 26 (7%) HIV mono-infected died. In the adjusted analysis, HIV-HBV co-infected group had a 2.53 times increased hazard of death (aHR: 2.52; 95% CI: 1.31-4.85) than HIV mono-infected. Conclusion: In this cohort study, mortality is higher in the HIV-HBV co-infected group. Hence, special attention shall be given to HIV-HBV co-infected groups, to significantly reduce mortality, and contribute to alleviating public health burden.
VL - 11
IS - 1
ER -
Copy
|
Download