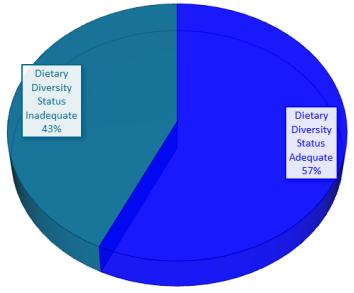
Introduction: Dietary diversity ensures that pregnant women consume the necessary range of nutrients from various food groups for the best possible outcomes for maternal health. Maternal health and fetal development are weakened by nutrient deficits caused by inadequate dietary diversity, typified by income constraints, and frequently restricted consumption of varied food categories. This study aimed to assess pregnant women's dietary diversity and household income status in Mbulu district, Tanzania. Methods: A cross-sectional study design was used among 384 pregnant women. Pregnant women were selected by using a systematic random sampling method. Eight health facilities were selected using a purposive sampling method. Face-to-face interviews were conducted by trained enumerators using a structured questionnaire that was divided into three sections to collect information on (i) socio-demographic characteristics, (ii) Dietary diversity, and (iii) Household income status. The Pearson Chi-square test and Logistic regression analysis were used to compare and test the association of dietary diversity and household income status to pregnant women's characteristics. Dietary diversity was evaluated using the Minimum Dietary Diversity Score (MDDS), while household income status was measured through income and expenditure data. Results: The findings revealed that about 43% of pregnant women had inadequate dietary diversity, while 57% had adequate dietary diversity. Dietary diversity was significantly associated with residential location areas (p = 0.016), education level (p = 0.045), and family size (p= 0.041). Results from logistic regression analysis showed that dietary diversity was associated with having residence in rural Mbulu district areas (OR = 0.357, p-value < 0.003), having a secondary education level (OR = 3.958, p-value < 0.007) and no formal education (OR = 1.122, p-value < 0.02), having average monthly household Income (OR = 4.934, p-value < 0.000) and husband (male partner) support (OR = 3.713, p-value < 0.001). Additionally, results from Chi-square test an average monthly household income (p = 0.001), food budget expenditure (p = 0.018), and food expenditure ability (p =0.000) were significantly associated with dietary diversity among pregnant women (p < 0.05). Conclusion: In this study, forty-three pregnant women had inadequate dietary diversity due to lower-income household level restricting access to diverse and nutritious food groups. Therefore, policymakers should encourage more dietary diversity and general maternal health requirements to raise sustainable household income-generating activities and improve nutrition education programs.
| Published in | Journal of Food and Nutrition Sciences (Volume 13, Issue 2) |
| DOI | 10.11648/j.jfns.20251302.11 |
| Page(s) | 48-63 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Dietary Diversity, Household Monthly Income, Pregnant Women, Maternal Health, Mbulu District Tanzania
Variable Category | Number of Respondents | Percent | |
|---|---|---|---|
Location | Rural | 190 | 49.5 |
Urban | 194 | 50.5 | |
Age (years) | 18-24 | 158 | 41.1 |
25-40 | 219 | 57.0 | |
≥41 | 7 | 1.8 | |
Marital Status | Cohabiting | 23 | 6.0 |
Divorced | 2 | 0.5 | |
Married | 304 | 79.2 | |
Single | 53 | 13.8 | |
Widowed | 2 | 0.5 | |
Education Level | No formal education | 11 | 2.9 |
Primary school | 246 | 64.1 | |
Secondary school | 109 | 28.4 | |
College or University | 18 | 4.7 | |
Occupation | Employed for wage | 10 | 2.6 |
Farmer | 323 | 84.1 | |
Pastoralist | 2 | 0.5 | |
Self-employed | 42 | 10.9 | |
Unemployed | 7 | 1.8 | |
Family Size (members) | <2 | 57 | 14.8 |
3-5 | 186 | 48.4 | |
>5 | 141 | 36.7 | |
Monthly Household Income (TZS) | < 250,000/= | 152 | 39.6 |
250,000-500,000/= | 158 | 41.1 | |
>500,000/= | 74 | 19.3 | |
Religion | Christian | 374 | 97.4 |
Muslim | 10 | 2.6 | |
Husband (Partner) Supports | No | 50 | 13.0 |
Yes | 334 | 87.0 | |
Variable Category | Dietary Diversity Status | Total (N= 384) | χ2 | Df | p-value | ||
|---|---|---|---|---|---|---|---|
Adequate =n (%) | Inadequate =n (%) | ||||||
Location | Rural | 120 (63.2) | 70 (36.8) | 190 | 5.761 | 1 | 0.016 |
Urban | 99 (51) | 95 (49) | 194 | ||||
Age (years) | 18-24 | 76 (48.1) | 82 (51.9) | 158 | 3.355 | 2 | 0.19 |
25-40 | 123 (56.2) | 96 (43.8) | 219 | ||||
≥41 | 5 (71.4) | 2 (28.6) | 7 | ||||
Marital Status Education Level | Cohabiting | 12 (52.2) | 11 (47.8) | 23 | |||
Divorced | 1 (50) | 1 (50) | 2 | 0.081 | 4 | 0.90 | |
Married | 161 (53) | 143 (47) | 304 | ||||
Single | 29 (54.7) | 24 (45.3) | 53 | ||||
Widowed | 1 (50) | 1 (50) | 2 | ||||
No formal education | 4 (40) | 6 (60) | 10 | 7.738 | 4 | 0.045 | |
Primary school | 125 (49.4) | 128 (50.6) | 253 | ||||
Secondary school | 61 (59.2) | 42 (40.8) | 103 | ||||
College or University | 14 (77.8) | 4 (22.2) | 18 | ||||
Occupation | Employed | 7 (70) | 3 (30) | 10 | |||
Farmer | 163 (50.5) | 160 (49.5) | 323 | ||||
Pastoralist | 2 (100) | 0 (0.00) | 2 | 6.965 | 4 | 0.138 | |
Self-employed | 28 (66.7) | 14 (33.3) | 42 | ||||
Unemployed | 4 (57.1) | 3 (42.9) | 7 | ||||
Family Size | <2 | 39 (68.4) | 18 (31.6) | 57 | |||
3-5 | 95 (51.1) | 91 (48.9) | 186 | 6.355 | 2 | 0.041 | |
>5 | 70 (49.6) | 71 (50.4) | 141 | ||||
Religion | Christian | 198 (52.9) | 176 (47.1) | 374 | 0.195 | 1 | 0.658 |
Muslim | 6 (60) | 4 (40) | 10 | ||||
Husband (Partner) Support | No | 25 (50) | 25 (50) | 50 | 225 | 1 | 0.635 |
Yes | 179 (53.6) | 155 (46.4) | 334 | ||||
Type of food group | Category | Frequency (N) | Percentage (%) | Location | p-value | |
|---|---|---|---|---|---|---|
Rural =n (%) | Urban =n (%) | |||||
Dietary Diversity Status | Adequate | 219 | 57.0 | 120 (54.8) | 99 (45.2) | 0.016 |
Inadequate | 165 | 43.0 | 70 (42.4) | 95 (57.6) | ||
Pulses (beans, peas and lentils) | No | 153 | 39.8 | 80 (53.3) | 73 (47.7) | 0.370 |
Yes | 231 | 60.2 | 110 (47.6) | 121 (52.4) | ||
Nuts and seeds | No | 215 | 56 | 76 (35.3) | 139 (64.7) | 0.000 |
Yes | 169 | 44 | 114 (67.5) | 55 (32.5) | ||
Milk and milk products | No | 111 | 28.9 | 41 (36.9) | 70 (63.1) | 0.002 |
Yes | 273 | 71.1 | 149 (54.6) | 124 (45.4) | ||
Meat, poultry, and fish | No | 246 | 64.1 | 113 (45.9) | 133 (54.1) | 0.064 |
Yes | 138 | 35.9 | 77 (55.8) | 61 (44.2) | ||
Eggs | No | 297 | 77.3 | 131 (44.1) | 166 (55.9) | 0.000 |
Yes | 87 | 22.7 | 59 (67.8) | 28 (32.2) | ||
Dark green leafy vegetables | No | 82 | 21.4 | 39 (47.6) | 43 (52.4) | 0.695 |
Yes | 302 | 78.6 | 151 (50) | 151 (50) | ||
Other fruits | No | 134 | 34.9 | 75 (56) | 59 (44) | 0.063 |
Yes | 250 | 65.1 | 115 (46) | 135 (54) | ||
Other vegetables | No | 181 | 47.1 | 71 (39.2) | 110 (60.8) | 0.000 |
Yes | 203 | 52.9 | 119 (58.6) | 84 (41.4) | ||
Other vitamin A-rich fruits and vegetables | No | 205 | 53.4 | 124 (60.5) | 81 (39.5) | 0.000 |
Yes | 179 | 46.6 | 66 (36.9) | 113 (63.1) | ||
Grains, white roots and tubers, and plantain | No | 10 | 3 | 4 (40) | 6 (60) | 0.544 |
Yes | 374 | 97.4 | 186 (49.7) | 188 (50.3) | ||
Household Income Status | Category | Location (Residents) | p-value | Dietary Diversity Status | Total | p-value | ||
|---|---|---|---|---|---|---|---|---|
Rural =n (%) | Urban = n (%) | Adequate =n (%) | Inadequate =n (%) | |||||
The main source of household income | Government employment | (20) | (80) | 0.022 | (70) | (30) | 10 | 0.138 |
Agriculture | 171 (52.6) | 154 (47.4) | 16 (50.8) | 16 (49.2) | 325 | |||
Business | 15 (35.7) | 2 (64.3) | 2 (66.7) | 1 (33.3) | 42 | |||
Others | 2 (28.6) | 5 (71.4) | (57.1) | (42.9) | 7 | |||
Average monthly household income (TZS) | 250,000-500,000/= | 67 (42.4) | 9 (57.6) | 0.039 | 7 (50.0) | 7 (50) | 158 | 0.001 |
<250,000/= | 79 (52) | 7 (48) | 10 (68.4) | 4 (31.6) | 152 | |||
>500,000/= | 4 (59.5) | 3 (40.5) | 3 (48.6) | 3 (51.4) | 74 | |||
Household Food expenditure per day | <5000 | 7 (38.9) | 11 (61.1) | 0.000 | 10 (56.8) | 8 (43.2) | 185 | 0.169 |
>5000 | 11 (59.3) | 8 (40.7) | 9 (49.7) | 10 (50.3) | 199 | |||
Monthly income percentage for food expenses | 10-25% | (14) | 3 (86) | 0.000 | 2 (62.8) | 1 (37.2) | 43 | 0.352 |
26-40% | (15) | 3 (85) | 2 (57.5) | 1 (42.5) | 40 | |||
unknown | (19.2) | 2 (80.8) | 1 (53.8) | 1 (46.2) | 26 | |||
< 10% | (20) | (80) | (20) | (80) | 5 | |||
> 50% | 17 (63.7) | 9 (36.3) | 13 (51.5) | 13 (48.5) | 270 | |||
Household Food budget expenses | No | 15 (55.1) | 124 (44.9) | 0.000 | 15 (56.9) | 11 (43.1) | 276 | 0.018 |
Yes | 3 (35.2) | 7 (64.8) | 4 (43.5) | 6 (56.5) | 108 | |||
Household Income Experience | No | 105 (44.7) | 130 (55.3) | 0.018 | 14 (59.6) | 9 (40.4) | 235 | 0.001 |
Yes | 85 (57) | 6 (43) | 6 (43) | 8 (57) | 149 | |||
Food budget adjustments | No | 12 (49.4) | 13 (50.6) | 0.974 | 15 (58.3) | 10 (41.7) | 259 | 0.003 |
Yes | 62 (49.6) | 63 (50.4) | 5 (42.4) | 7 (57.6) | 125 | |||
Food expenditure ability to purchase | No | 104 (46.6) | 119 (53.4) | 0.19 | 13 (62.3) | 8 (37.7) | 223 | 0.000 |
Yes | 86 (53.4) | 75 (46.6) | 6 (40.4) | 9 (59.6) | 161 | |||
The government assistance (IFAS) | No | 47 (85.5) | 8 (14.5) | 0.000 | 3 (67.3) | 1 (32.7) | 55 | 0.023 |
Yes | 143 (43.5) | 186 (56.5) | 16 (50.8) | 16 (49.2) | 329 | |||
Variable | Odds ratio | df | Sig. | 95% C.I.for Odds | |
|---|---|---|---|---|---|
Lower | Upper | ||||
Location (District -Rural) | 0.357 | 1 | 0.003 | 0.182 | 0.701 |
Age group | 2 | 0.865 | |||
18-24 years | 0.775 | 1 | 0.812 | 0.094 | 6.377 |
25-40 years | 0.898 | 1 | 0.919 | 0.113 | 7.105 |
Marital status | 4 | 0.107 | |||
Cohabiting | 0.87 | 1 | 0.878 | 0.147 | 5.156 |
Divorced | 4.162 | 1 | 0.435 | 0.116 | 149.165 |
Married | 1.132 | 1 | 0.873 | 0.247 | 5.183 |
Single | 2.668 | 1 | 0.221 | 0.555 | 12.833 |
Education Level for Pregnant Women | 4 | 0.000 | |||
No formal education | 0.122 | 1 | 0.021 | 0.02 | 0.726 |
Primary school | 0.918 | 1 | 0.866 | 0.343 | 2.458 |
Secondary school | 3.958 | 1 | 0.007 | 1.457 | 10.752 |
High school/Certificate/Diploma | 0.75 | 1 | 0.529 | 0.307 | 1.835 |
Occupation | 4 | 0.000 | |||
Employed | 1.25 | 1 | 0.840 | 0.144 | 10.859 |
Farmer | 0.67 | 1 | 0.694 | 0.091 | 4.938 |
Pastoralist | 3.599 | 1 | 0.272 | 0.367 | 35.329 |
Self-employed | 3.823 | 1 | 0.202 | 0.487 | 29.997 |
Average monthly household income | 2 | 0.000 | |||
< 250,000/= | 4.934 | 1 | 0.000 | 2.283 | 10.662 |
250,000/= - 500,000/= | 1.009 | 1 | 0.978 | 0.521 | 1.957 |
Parity | 2 | 0.077 | |||
< 2 | 1.364 | 1 | 0.535 | 0.512 | 3.637 |
3-5 parities | 0.584 | 1 | 0.207 | 0.253 | 1.347 |
Family Size | 2 | 0.216 | |||
< 2 | 0.581 | 1 | 0.081 | 0.316 | 1.069 |
3-5 members | 0.674 | 1 | 0.373 | 0.283 | 1.606 |
Religion (Christian) | 0.637 | 1 | 0.246 | 0.298 | 1.364 |
Husband (Male Partner) Support (Yes) | 3.713 | 1 | 0.001 | 1.722 | 8.006 |
Constant | 0.534 | 1 | 0.709 | ||
LMICs | Low and Middle-Income Countries |
WHO | World Health Organization |
FAO | Food and Agriculture Organization |
MDD-W | Minimum Dietary Diversity for Women |
NBS | National Bureau Statistics |
MoHCDGEC | Ministry of Health, Community Development, Gender, Elderly and Children |
TDHS-MIS | Tanzania Demographic Health Survey and Malaria Indicator Survey |
| [1] | FAO, UNICEF, WFP and WHO. 2021. Asia and the Pacific Regional Overview of Food Security and Nutrition 2020: Maternal and child diets at the heart of improving nutrition. Bangkok, FAO. |
| [2] | Puliani, R., Bhatt, Y., Gupta, S., & Jayanna, K. (2024). A Scoping Review of Barriers and Facilitators for Preconception Care: Lessons for Global Health Policies and Programs. Asia Pacific Journal of Public Health, 10105395241252867. |
| [3] | Alaoui, E. H. (2023). Socio-economic inequalities, gender and malnutrition in developing countries (Doctoral dissertation, Université de Bordeaux). |
| [4] | Clark, H., Coll-Seck, A. M., Banerjee, A., Peterson, S., Dalglish, S. L., Ameratunga, S.,... & Costello, A. (2020). A future for the world's children? A WHO–UNICEF–Lancet Commission. The Lancet, 395(10224), 605-658. |
| [5] | Tholandi, M., Zethof, S., Kim, Y. M., Tura, A. K., Ket, J., Willcox, M., & Ilozumba, O. (2024). Approaches to improve and adapt maternal mortality estimations in low-and middle-income countries: A scoping review. International Journal of Gynecology & Obstetrics, 165(1), 94-106. |
| [6] | Habte, A., Bizuayehu, H. M., Lemma, L., & Sisay, Y. (2024). Road to maternal death: the pooled estimate of maternal near-miss, its primary causes and determinants in Africa: a systematic review and meta-analysis. BMC Pregnancy and Childbirth, 24(1), 144. |
| [7] | Anaemia - World Health Organization (WHO). (2025). |
| [8] | Rainford, M., Barbour, L. A., Birch, D., Catalano, P., Daniels, E., Gremont, C., & Thornburg, K. (2024). Barriers to implementing good nutrition in pregnancy and early childhood: Creating equitable national solutions. Annals of the New York Academy of Sciences, 1534(1), 94-105. |
| [9] | Forestell, C. A. (2024). Does Maternal Diet Influence Future Infant Taste and Odor Preferences? A Critical Analysis. Annual Review of Nutrition, 44. |
| [10] | World Health Organization. (2018). Minimum dietary diversity for women: A measurement guide. Geneva: World Health Organization. |
| [11] | FAO. (2021). Minimum Dietary Diversity for Women: A Guide to Measurement. Food and Agriculture Organization of the United Nations. Rome. |
| [12] | Heri, R., Malqvist, M., Yahya-Malima, K. I., & Mselle, L. T. (2024). Dietary diversity and associated factors among women attending antenatal clinics in the coast region of Tanzania. BMC nutrition, 10(1), 16. |
| [13] | Kebede, A. N., Sahile, A. T., & Kelile, B. C. (2022). Dietary diversity and associated factors among pregnant women in Addis Ababa, Ethiopia, 2021. International Journal of Public Health, 67, 1605377. |
| [14] | Shamim, A. A., Mashreky, S. R., Ferdous, T., Tegenfeldt, K., Roy, S., Rahman, A. F., & Shaheen, N. (2016). Pregnant women's diet quality and its socio-demographic determinants in southwestern Bangladesh. Food and Nutrition Bulletin, 37(1), 14-26. |
| [15] | Tilahun, A. G., & Kebede, A. M. (2021). Maternal minimum dietary diversity and associated factors among pregnant women, Southwest Ethiopia, 2021. BMC Nutrition 7, 1-10. |
| [16] | Yang, J., Wang, M., Tobias, D. K., Rich-Edwards, J. W., Darling, A. M., Abioye, A. I., & Fawzi, W. W. (2022). Dietary diversity and diet quality with gestational weight gain and adverse birth outcomes results from a prospective pregnancy cohort study in urban Tanzania. Maternal & child nutrition, 18(2), e13300. |
| [17] | Madzorera, I., Isanaka, S., Wang, M., Msamanga, G. I., Urassa, W., Hertzmark, E., & Fawzi, W. W. (2020). Maternal dietary diversity and dietary quality scores in relation to adverse birth outcomes in Tanzanian women. The American Journal of Clinical Nutrition, 112(3), 695-706. |
| [18] | Nazni, P., Darki, H. S., Aliyu, H. I., Umar, A. M., & Kura, Y. S. (2023). Basic Food Groups’ Consumption Pattern Among Pregnant Women: Food Consumption Among Pregnant Women. Journal of Food and Dietetics Research, 3(1), 24-28. |
| [19] | Alemayehu, M. S., & Tesema, E. M. (2015). Dietary practice and associated factors among pregnant women in Gondar north t, Ethiopia, 2014. Int J Nutr Food Sci, 4(6), 707-712. |
| [20] | Thompson, K. L. (2024). Nutrition In Pregnancy: Population Health Perspectives. Life Cycle Nutrition for Public Health Professionals, 47. |
| [21] | Wondmeneh, T. G. (2022). Dietary diversity practice and its influencing factors among pregnant women in Afar region of Ethiopia: mixed method study. BMC Pregnancy and Childbirth, 22(1), 291. |
| [22] | FAO. (2024). State of Food Security and Nutrition in the World. Food and Agriculture Organization of the United Nations. |
| [23] | Madzorera, I., Blakstad, M. M., Bellows, A. L., Canavan, C. R., Mosha, D., Bromage, S.,... & Fawzi, W. W. (2021). Food crop diversity, women's income-earning activities, and distance to markets in relation to maternal dietary quality in Tanzania. The Journal of Nutrition, 151(1), 186-196. |
| [24] | Hawkes, C., Harris, J., & Gillespie, S. (2017). "Urbanization and the Nutrition Transition." In Global Food Policy Report 2017 (pp. 34-41). IFPRI. |
| [25] | Kinabo, J., Haug, A., Rukoa, E., & Gondwe, T. (2017). "Food Variety, Dietary Diversity, and Nutritional Status of Women and Children in Tanzania." Ecology of Food and Nutrition, 56(2), 134-152. |
| [26] | United Nations International Children's Emergency Fund (UNICEF). (2019). Nutrition in Africa. Retrieved from UNICEF. |
| [27] | World Food Programme (WFP). (2020). Tanzania. Retrieved from WFP. |
| [28] | Seid, A., Dugassa Fufa, D., Weldeyohannes, M., Tadesse, Z., Fenta, S. L., Bitew, Z. W., & Dessie, G. (2023). Inadequate dietary diversity during pregnancy increases the risk of maternal anaemia and low birth weight in Africa: A systematic review and meta-analysis. Food Science & Nutrition, 11(7), 3706-3717. |
| [29] | Beressa, G., Whiting, S. J., & Belachew, T. (2024). Effect of nutrition education integrating the health belief model and theory of planned behaviour on dietary diversity of pregnant women in Southeast Ethiopia: a cluster randomized controlled trial. Nutrition Journal, 23(1), 3. |
| [30] | Uwase, A., Nsereko, E., Pillay, N., & Levin, J. (2024). Dietary diversity and associated factors among pregnant women in the Southern Province of Rwanda: A facility-based cross-sectional study. Plos one, 19(2), e0297112. |
| [31] | Katenga-Kaunda, L. Z. (2023). Nutrition education and counselling to enhance dietary diversity among pregnant women in rural Malawi. |
| [32] | Dewidar, O., John, J., Baqar, A., Madani, M. T., Saad, A., Riddle, A.,... & Welch, V. (2023). Effectiveness of nutrition counseling for pregnant women in low-and middle-income countries to improve maternal and infant behavioral, nutritional, and health outcomes: A systematic review. Campbell Systematic Reviews, 19(4), e1361. |
| [33] | Geta, T. G., Gebremedhin, S., & Omigbodun, A. O. (2022). Dietary diversity among pregnant women in Gurage Zone, South Central Ethiopia: assessment based on longitudinal repeated measurement. International Journal of Women's Health, 599-615. |
| [34] | Alemu, F. T., Desta, A. A., & Tola, A. G. (2024). Dietary diversity and associated factors among pregnant women attending antenatal care at public hospitals in North Shewa, Oromia, Ethiopia, 2023. Frontiers in Nutrition, 11, 1400813. |
| [35] | Ministry of Finance and Planning, Tanzania National Bureau of Statistics and President's Office - Finance and Planning, Office of the Chief Government Statistician, Zanzibar. The 2022 Population and Housing Census: Age and Sex Distribution Report Tanzania Mainland, December 2022. |
| [36] | Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC). (2016). Tanzania Demographic and Health Survey and Malaria Indicator Survey 2015-2016. MoHCDGEC. |
| [37] | World Bank. (2018). Tanzania Economic Update: The Power of Investing in Girls. World Bank Group. |
| [38] | Brydges, C. R. (2019). Effect size guidelines, sample size calculations, and statistical power in gerontology. Innovation in Aging, 3(4), igz036. |
| [39] | Shrestha, V., Paudel, R., Sunuwar, D. R., Lyman, A. L. T., Manohar, S., Amatya, A. (2021). Factors associated with dietary diversity among pregnant women in the western hill region of Nepal: a community-based cross-sectional study PLoS One. 2021; 16(4): e0247085. |
| [40] | Tesfaye, A., Gerbaba, M., Tamiru, D., & Belachew, T. (2024). Inadequate dietary diversity practices and associated factors among pregnant adolescents in the West Arsi Zone, Central Ethiopia: a community-based cross-sectional study. Scientific Reports, 14(1), 2871. |
| [41] | Olatona, F. A., Olowu, O. J., Goodman, O. O., & Amu, E. O. (2021). Dietary habits, diversity, and predictors among pregnant women attending primary health care centers for antenatal care in Lagos, Nigeria. Journal of Family Medicine and Primary Care, 10(8), 3076-3083. |
| [42] | Delil, R., Zinab, B., Mosa, H., Ahmed, R., & Hassen, H. (2021). Determinants of dietary diversity practice among pregnant women attending antenatal clinic at Wachemo University Nigist Eleni Mohammed Memorial referral Hospital Southern Ethiopia. PLoS One. 16(4): e0250037. PMID: 33836030 PLOS ONE Dietary diversity among pregnant women of Rwanda's Southern ProvincePLOS. |
| [43] | Shenka, A., Damena, M., Abdo, M., & Roba, K. T. (2018). Dietary Diversity and Nutritional Status of Pregnant Women Attending Public Hospitals in Dire Dawa City Administration, Eastern Ethiopia. East African Journal of Health and Biomedical Sciences, 2018; 2(1): 10–7. |
| [44] | Hidru, H. D., Berwo Mengesha, M., Hailesilassie, Y., & Tekulu Welay, F. (2020). Burden and determinant of inadequate dietary diversity among pregnant women in Ethiopia: A systematic review and meta-analysis. Journal of Nutrition and Metabolism, 2020(1), 1272393. |
| [45] | Ochieng, J., Afari-Sefa, V., Lukumay, P. J., & Dubois, T. (2017). Determinants of Dietary Diversity and the Potential Role of Men in Improving Household Nutrition in Tanzania. PloS one 12(12): e0189022. |
| [46] | Kiboi, W., Kimiywe, J., & Chege, P. (2016). Dietary Diversity, Nutrient Intake and Nutritional Status among Pregnant Women in Laikipia County, Kenya. International Journal of Health Sci Res 6, 378–9. |
| [47] | Demilew, Y. M., Alene, G. D., & Belachew, T. (2020). Dietary Practices and Associated Factors Among Pregnant Women in West Gojjam Zone, Northwest Ethiopia. BMC Pregnancy Childbirth 20(1), 18–1. |
| [48] | Gudeta, T. G., Terefe, A. B., Mengistu, G. T., Sori, S. A. (2022). Determinants of dietary diversity practice among pregnant women in the Gurage Zone, Southern Ethiopia, 2021: Community-based cross-sectional study. Obstet Gynecol Int. 2022; 2022: 8086793. |
| [49] | Tefera, W., Brhanie, T. W., & Dereje, M. (2020). Dietary diversity practice and associated factors among pregnant women attending ANC in Kolfe Keranyo sub-city health centres, Addis Ababa, Ethiopia. medRxiv, 2020-04. |
| [50] | Yeneabat, T., Adugna, H., Asmamaw, T., Wubetu, M., Admas, M., Hailu, G., & Amare, T. (2019). Maternal dietary diversity and micronutrient adequacy during pregnancy and related factors in East Gojjam Zone, Northwest Ethiopia, 2016. BMC pregnancy and childbirth, 19, 1-9. |
| [51] | Aliwo, S., Fentie, M., Awoke, T., & Gizaw, Z. (2019). Dietary diversity practice and associated factors among pregnant women in North East Ethiopia. BMC research notes. 12(1), 1–6. |
| [52] | Hailu, S., & Woldemichael, B. (2019). Dietary diversity and associated factors among pregnant women attending antenatal care at public health facilities in Bale zone. Southeast Ethiopia Nutrition and Dietary Supplements. 2019; 11, 1–8. |
| [53] | Desta, M., Akibu, M., Tadese, M., & Tesfaye, M. (2019). Dietary Diversity and Associated Factors Among Pregnant Women Attending Antenatal Clinic in Shashemane, Oromia, Central Ethiopia: A cross-sectional study. Journal of nutrition and metabolism, 2019(1), 3916864. |
| [54] | Ministry of Health (MoH) [Tanzania Mainland], Ministry of Health (MoH) [Zanzibar], National Bureau of Statistics (NBS), Office of the Chief Government Statistician (OCGS), and ICF. 2022. Tanzania Demographic and Health Survey and Malaria Indicator Survey 2022 Final Report. Dodoma, Tanzania, and Rockville, Maryland, USA: MoH, NBS, OCGS, and ICF. |
| [55] | Konje, E. T., Ngaila, B. V., Kihunrwa, A., Mugassa, S., Basinda, N., & Dewey, D. (2022). High prevalence of anaemia and poor compliance with preventive strategies among pregnant women in Mwanza City, Northwest Tanzania: a hospital-based cross-sectional study. Nutrients, 14(18), 3850. |
| [56] | Delil, R., Tamiru, D., & Zinab, B. (2018). Dietary diversity and its association with anaemia among pregnant women attending public health facilities in South Ethiopia. Ethiopian journal of health sciences, 28(5). |
| [57] | Twum-Dei, B., Aryeetey, R., & Aduku, L. N. E. (2024). Dietary diversity and preferences among pregnant women and its association with anaemia. Nutrition & Food Science. |
| [58] | Jemal, K., & Awol, M. (2019). Minimum dietary diversity score and associated factors among pregnant women at Alamata General Hospital, Raya Azebo Zone, Tigray Region, Ethiopia. Journal of nutrition and metabolism, 2019(1), 8314359. |
| [59] | Amugsi, D. A., Lartey, A., Kimani-Murage, E., & Mberu, B. U. (2016). Women's Participation in Household Decision-Making and Higher Dietary Diversity: Findings from Nationally Representative Data from Ghana. Journal of Health Population Nutrition 35(1), 16–8. |
| [60] | Kiboi, W., Kimiywe, J., & Chege, P. (2017). Determinants of Dietary Diversity Among Pregnant Women in Laikipia County, Kenya: a Cross-Sectional Study. BMC Nutr 3(1), 12–8. |
| [61] | Kimuli, D., Nakaggwa, F., Namuwenge, N., Nsubuga, R. N., Kasule, K., Nyakwezi, S., & Bukenya, D. (2024). Prevalence and determinants of minimum dietary diversity for women of reproductive age in Uganda. BMC nutrition, 10(1), 39. |
| [62] | NYAMASEGE, C. K. (2021). Effects of Maternal Nutrition Education on Children's Nutrition and Health in Nairobi, Kenya. |
| [63] | Gebremichael, M. A., & Belachew Lema, T. (2023). Dietary Diversity, Nutritional Status, and Associated Factors Among Pregnant Women in Their First Trimester of Pregnancy in Ambo District, Western Ethiopia. Nutrition and Metabolic Insights, 16, 11786388231190515. |
| [64] | FAO. (2021). The State of Food Security and Nutrition in the World. Rome: FAO. |
| [65] | Onyeji, G. N., & Sanusi, R. A. (2020). Dietary diversity of reproductive age women in three South-Eastern States of Nigeria. African Journal of Food, Agriculture, Nutrition and Development, 20(2), 15490-15508. |
| [66] | Mekonen, H. (2020). Dietary diversity and associated factors among pregnant women in east belessa district, central gondar, ethiopia: community based cross-sectional study (Doctoral dissertation). |
| [67] | World Bank. (2023). Global economic Prospects, January 2023. Washington, DC. |
| [68] | Issa, M. Y., Diagana, Y., Khalid, E. K., Coulibaly, S. M., Gueye, A., Dehah, R. M., & Vall, O. E. K. M. (2024). Dietary diversity and its determinants among women of reproductive age residing in the urban area of Nouakchott, Mauritania. BMC Public Health, 24(1), 916. |
| [69] | Gartaula, H. N., Atreya, K., Kattel, K., & Rahut, D. B. (2024). Factors influencing household and women’s dietary diversity in migrant households in central Nepal. Plos one, 19(4), e0298022. |
| [70] | Mesfin, A. M., Deribo, T., Demissie, W. R., & Neme, K. (2024). Dietary diversity status and its associated factors among pregnant women in Fedis Woreda of East Hararghe Zone, Oromia Regional State, Ethiopia: A community-based cross-sectional study. |
| [71] | Akinyi, M. P., & Esther, M. A. (2024). Factors Influencing Dietary Practices of Pregnant Women at Njoro Sub County Hospital, Nakuru County, Kenya. Current Research in Medical Sciences, 3(2), 76-82. |
| [72] | Oliveira, T. I. D., Santos, L. D., & Höfelmann, D. A. (2023). Dietary patterns and socioeconomic, demographic and health-related behaviours during pregnancy. A cross-sectional study. Sao Paulo Medical Journal, 142, e2022629. |
| [73] | Nguyen, P. H., Frongillo, E. A., Sanghvi, T., Wable, G., Mahmud, Z., Tran, L. M.,... & Menon, P. (2018). Engagement of husbands in a maternal nutrition program substantially contributed to greater intake of micronutrient supplements and dietary diversity during pregnancy: results of a cluster-randomized program evaluation in Bangladesh. The Journal of Nutrition, 148(8), 1352-1363. |
APA Style
Hudson, P., Muhimbula, H., Mosha, T. (2025). Dietary Diversity and Household Income Status Among Pregnant Women in Mbulu District, Tanzania. Journal of Food and Nutrition Sciences, 13(2), 48-63. https://doi.org/10.11648/j.jfns.20251302.11
ACS Style
Hudson, P.; Muhimbula, H.; Mosha, T. Dietary Diversity and Household Income Status Among Pregnant Women in Mbulu District, Tanzania. J. Food Nutr. Sci. 2025, 13(2), 48-63. doi: 10.11648/j.jfns.20251302.11
@article{10.11648/j.jfns.20251302.11,
author = {Paul Hudson and Happiness Muhimbula and Theobald Mosha},
title = {Dietary Diversity and Household Income Status Among Pregnant Women in Mbulu District, Tanzania
},
journal = {Journal of Food and Nutrition Sciences},
volume = {13},
number = {2},
pages = {48-63},
doi = {10.11648/j.jfns.20251302.11},
url = {https://doi.org/10.11648/j.jfns.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jfns.20251302.11},
abstract = {Introduction: Dietary diversity ensures that pregnant women consume the necessary range of nutrients from various food groups for the best possible outcomes for maternal health. Maternal health and fetal development are weakened by nutrient deficits caused by inadequate dietary diversity, typified by income constraints, and frequently restricted consumption of varied food categories. This study aimed to assess pregnant women's dietary diversity and household income status in Mbulu district, Tanzania. Methods: A cross-sectional study design was used among 384 pregnant women. Pregnant women were selected by using a systematic random sampling method. Eight health facilities were selected using a purposive sampling method. Face-to-face interviews were conducted by trained enumerators using a structured questionnaire that was divided into three sections to collect information on (i) socio-demographic characteristics, (ii) Dietary diversity, and (iii) Household income status. The Pearson Chi-square test and Logistic regression analysis were used to compare and test the association of dietary diversity and household income status to pregnant women's characteristics. Dietary diversity was evaluated using the Minimum Dietary Diversity Score (MDDS), while household income status was measured through income and expenditure data. Results: The findings revealed that about 43% of pregnant women had inadequate dietary diversity, while 57% had adequate dietary diversity. Dietary diversity was significantly associated with residential location areas (p = 0.016), education level (p = 0.045), and family size (p= 0.041). Results from logistic regression analysis showed that dietary diversity was associated with having residence in rural Mbulu district areas (OR = 0.357, p-value p =0.000) were significantly associated with dietary diversity among pregnant women (p Conclusion: In this study, forty-three pregnant women had inadequate dietary diversity due to lower-income household level restricting access to diverse and nutritious food groups. Therefore, policymakers should encourage more dietary diversity and general maternal health requirements to raise sustainable household income-generating activities and improve nutrition education programs.
},
year = {2025}
}
TY - JOUR T1 - Dietary Diversity and Household Income Status Among Pregnant Women in Mbulu District, Tanzania AU - Paul Hudson AU - Happiness Muhimbula AU - Theobald Mosha Y1 - 2025/03/07 PY - 2025 N1 - https://doi.org/10.11648/j.jfns.20251302.11 DO - 10.11648/j.jfns.20251302.11 T2 - Journal of Food and Nutrition Sciences JF - Journal of Food and Nutrition Sciences JO - Journal of Food and Nutrition Sciences SP - 48 EP - 63 PB - Science Publishing Group SN - 2330-7293 UR - https://doi.org/10.11648/j.jfns.20251302.11 AB - Introduction: Dietary diversity ensures that pregnant women consume the necessary range of nutrients from various food groups for the best possible outcomes for maternal health. Maternal health and fetal development are weakened by nutrient deficits caused by inadequate dietary diversity, typified by income constraints, and frequently restricted consumption of varied food categories. This study aimed to assess pregnant women's dietary diversity and household income status in Mbulu district, Tanzania. Methods: A cross-sectional study design was used among 384 pregnant women. Pregnant women were selected by using a systematic random sampling method. Eight health facilities were selected using a purposive sampling method. Face-to-face interviews were conducted by trained enumerators using a structured questionnaire that was divided into three sections to collect information on (i) socio-demographic characteristics, (ii) Dietary diversity, and (iii) Household income status. The Pearson Chi-square test and Logistic regression analysis were used to compare and test the association of dietary diversity and household income status to pregnant women's characteristics. Dietary diversity was evaluated using the Minimum Dietary Diversity Score (MDDS), while household income status was measured through income and expenditure data. Results: The findings revealed that about 43% of pregnant women had inadequate dietary diversity, while 57% had adequate dietary diversity. Dietary diversity was significantly associated with residential location areas (p = 0.016), education level (p = 0.045), and family size (p= 0.041). Results from logistic regression analysis showed that dietary diversity was associated with having residence in rural Mbulu district areas (OR = 0.357, p-value p =0.000) were significantly associated with dietary diversity among pregnant women (p Conclusion: In this study, forty-three pregnant women had inadequate dietary diversity due to lower-income household level restricting access to diverse and nutritious food groups. Therefore, policymakers should encourage more dietary diversity and general maternal health requirements to raise sustainable household income-generating activities and improve nutrition education programs. VL - 13 IS - 2 ER -
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Chuo Kikuu, Morogoro, Tanzania
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Chuo Kikuu, Morogoro, Tanzania
Department of Human Nutrition and Consumer Sciences, Sokoine University of Agriculture, Chuo Kikuu, Morogoro, Tanzania
Information