This study was conducted to determine association between perioperative antibiotic prophylaxis practices and occurrence of surgical site infections at Dodoma Regional Referral Hospital in Tanzania. Surgical site infections (SSIs) are preventable complications following surgery, but still cause significant burden in terms of patient morbidity, mortality and increased cost of treatment. A prospective cohort study was conducted among 162 operated patients. Patients with different trends of antibiotic prophylaxis were followed up for occurrence SSIs. Analysis of data was done by SPSS version 20 program using frequency tables, chi square test, Kaplan-meier and Cox regression methods. Significance level of < 0.05 was taken to establish associations between variables. It was found that, 60.5% of patients received preoperative antibiotic prophylaxis, the overall surgical site infections rate was 14.8%. There was no significant difference in occurrence of surgical site infections between patients who received and those who did not receive preoperative antibiotic prophylaxis (p=0.88). The study concluded that SSIs are significant complications. Perioperative antibiotic prophylaxis is commonly practiced. Establishment of local protocol on antibiotic prophylaxis and adherence to infection prevention can improve the prevailing situation.
| Published in | Journal of Surgery (Volume 12, Issue 2) |
| DOI | 10.11648/j.js.20241202.12 |
| Page(s) | 20-32 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Antibiotics, Perioperative, Prophylaxis, Surgical Site Infections
2.1. Design and Setting
2.2. Data Acquisition and Variables
2.3. Sampling and Analysis
3.1. Sociodemographic and Clinical Characteristics of the Cohort
Variables | Variable categories | n | % |
|---|---|---|---|
Age | Less than 5 years | 7 | 4.3 |
5years to less than18 years | 21 | 13.0 | |
18years to less than 60 years | 77 | 47.5 | |
More or equal to 60 years | 57 | 35.2 | |
Total | 162 | 100.0 | |
Sex | Male | 54 | 33.3 |
Female | 108 | 66.7 | |
Total | 162 | 100.0 | |
Education level | Formal education | 47 | 29.0 |
Primary education | 74 | 45.7 | |
Secondary education | 33 | 20.4 | |
Higher education | 8 | 4.9 | |
Total | 162 | 100.0 | |
Current smoking | Yes | 25 | 15.4 |
No | 137 | 84.6 | |
Total | 162 | 100.0 | |
Previous smoking | Yes | 32 | 23.5 |
No | 104 | 76.5 | |
Total | 136 | 100.0 | |
HIV status | Reactive | 11 | 9.2 |
Non-reactive | 108 | 90.8 | |
Total | 119 | 100.0 | |
SSI occurrence | Yes | 24 | 14.8 |
No | 138 | 85.2 | |
Total | 162 | 100.0 |
3.2. Perioperative Characteristics of Surgical Patients Who Underwent Surgeries
Variables | Variable categories | n | % |
|---|---|---|---|
Preoperative hospital stay | Less or equal 2days | 129 | 79.6 |
More than 2days | 25 | 15.4 | |
More or equal to 7days | 8 | 4.9 | |
Wound class | Clean | 70 | 43.2 |
Clean contaminated | 59 | 36.4 | |
Contaminated | 31 | 19.1 | |
Infected | 2 | 1.2 | |
Total | 162 | 100.0 | |
ASA score | I | 39 | 24.1 |
II | 93 | 57.4 | |
III | 29 | 17.9 | |
IV | 1 | .6 | |
Total | 162 | 100.0 | |
Use of drain | Yes | 63 | 38.9 |
No | 99 | 61.1 | |
Total | 162 | 100.0 | |
Blood transfusion | Yes | 11 | 6.8 |
No | 151 | 93.2 | |
Total | 162 | 100.0 | |
3-4days | 5 | 3.1 | |
More or equal to 5days | 150 | 92.6 | |
Total | 162 | 100.0 | |
Operation duration | 70 | 43.2 | |
72 | 44.4 | ||
<4hour | 20 | 12.3 | |
Types of operations | |||
Abdominal | 84 | 51.9 | |
Urological | 37 | 22.8 | |
Perineal | 9 | 5.6 | |
Biopsy | 10 | 6.2 | |
Chest | 4 | 2.5 | |
Neck | 4 | 2.5 | |
Others | 14 | 8.6 | |
Total | 162 | 100.0 | |
3.3. Antibiotic Prophylaxis Pattern Among Surgical Patients Who Underwent Surgeries
Variable | Variable Categories | n | % |
|---|---|---|---|
Preoperative antibiotics | Yes | 98 | 60.5 |
No | 64 | 39.5 | |
Total | 162 | 100.0 | |
Mode of preop-antibiotics | single | 97 | 99 |
multiple | 1 | 1 | |
Timing of antibiotics prophylaxis (preop) | within one hour | 79 | 94 |
more than one hour | 5 | 6 | |
Total | 88 | 100.0 | |
Intraoperative antibiotics | Yes | 14 | 8.8 |
No | 146 | 91.2 | |
Postoperative antibiotics | Total | 160 | 100 |
Yes | 160 | 98.8 | |
No | 2 | 1.2 | |
Total | 162 | 100.0 | |
Duration of post | 1day | 3 | 1.9 |
Operative antibiotics | 2days | 4 | 2.5 |
3-4days | 5 | 3.1 | |
More or equal to 5 days | 150 | 92.6 | |
Total | 162 | 100 | |
Antibiotic(s) | Ceft | 84 | 85.7 |
Ceft, Gent, Metr | 1 | 1.0 | |
Ceft, Metr | 13 | 13.3 | |
Total | 98 | 100.0 |
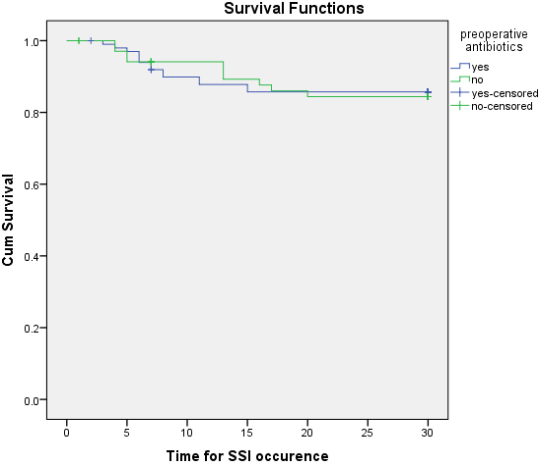
3.4. Means for Survival Time Between Patients Given Preoperative Antibiotic Prophylaxis and Patients Not Given Preoperative Antibiotic Prophylaxis
Means for Survival Time | p-value | ||||
|---|---|---|---|---|---|
preoperative antibiotics | Estimate | Std. Error | 95% Confidence Interval | ||
Lower Bound | Upper Bound | 0.88 | |||
yes | 26.863 | .787 | 25.320 | 28.407 | |
no | 27.072 | .885 | 25.336 | 28.808 | |
Overall | 26.953 | .590 | 25.796 | 28.109 | |
3.5. Relationship Between Wound Class and Preoperative Antibiotics Among Surgical Patients Who Underwent Surgeries
preoperative antibiotics | Total | P-value | |||
|---|---|---|---|---|---|
Yes | No | ||||
wound class | clean | 43 | 27 | 70 | 0.021 |
61.4% | 38.6% | 100.0% | |||
clean contaminated | 39 | 20 | 59 | ||
66.1% | 33.9% | 100.0% | |||
contaminated | 21 | 10 | 31 | ||
67.7% | 32.3% | 100.0% | |||
infected | 2 | 0 | 2 | ||
100.0% | 0.0% | 100.0% | |||
Total | 105 | 57 | 162 | ||
64.8% | 35.2% | 100.0% | |||
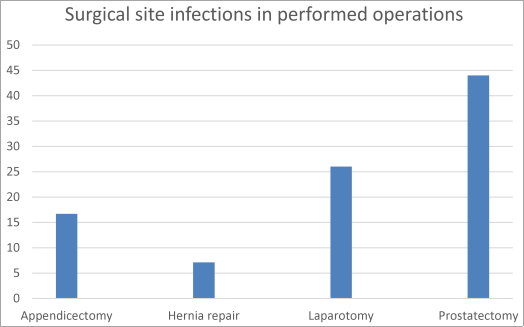
3.6. Surgical Site Infections by Type of Operations
3.7. Perioperative Antibiotics Administration
4.1. Surgical Site Infections Occurrence
4.2. Surgical Antibiotic Prophylaxis Pattern
4.3. Association Between Surgical Antibiotic Prophylaxis and Surgical Site Infections
| [1] | Horan, T. C., Gaynes, R. P., Martone, W. J., Jarvis, W. R., & Emori, T. G. (1992). CDC definitions of nosocomial surgical site infections, 1992: a modification of CDC definitions of surgical wound infections. American Journal of Infection Control, 20 (5), 271–4. Retrieved from |
| [2] | Martone, W. J., & Nichols, R. L. (2001). Recognition, Prevention, Surveillance, and Management of Surgical Site Infections: Introduction to the Problem and Symposium Overview. Clinical Infectious Diseases, 33 (s2), S67–S68. |
| [3] |
World Health Organization, (WHO). (2011). Report on the Burden of Endemic Health Care-Associated Infection Worldwide. WHO Library Cataloguing-in-Publication Data, 40.
http://whqlibdoc.who.int/publications/2011/9789241501507_eng.pdf |
| [4] | Magill, S. S., Edwards, J. R., Bamberg, W., Beldavs, Z. G., Dumyati, G., Kainer, M. A.,… Fridkin, S. K. (2014). Multistate Point-Prevalence Survey of Health Care–Associated Infections. New England Journal of Medicine, 370 (13), 1198–1208. |
| [5] | Gaynes, R. P., Culver, D. H., Horan, T. C., Edwards, J. R., Richards, C., & Tolson, J. S. (2001). Surgical Site Infection (SSI) Rates in the United States, 1992–1998: The National Nosocomial Infections Surveillance System Basic SSI Risk Index. Clinical Infectious Diseases, 33 (s2), S69–S77. |
| [6] | Gastmeier, P., Geffers, C., Brandt, C., Zuschneid, I., Sohr, D., Schwab, F.,… Rüden, H. (2006). Effectiveness of a nationwide nosocomial infection surveillance system for reducing nosocomial infections. The Journal of Hospital Infection, 64 (1), 16–22. |
| [7] | Odom-Forren, J. (2006). Preventing surgical site infections. Nursing, 36 (6), 58-63–4. Retrieved from |
| [8] | Allegranzi, B., Bischoff, P., de Jonge, S., Kubilay, N. Z., Zayed, B., Gomes, S. M.,… Solomkin, J. S. (2016). New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. The Lancet Infectious Diseases, 16 (12), e276–e287. |
| [9] | Nejad, S. B., Allegranzi, B., Syed, S. B., & Pittet, D. (2011). Health-care-associated infection in Africa : a systematic review, (March), 757–765. |
| [10] | Mulu, W., Kibru, G., Beyene, G., & Damtie, M. (2013). Associated Risk factors for Postoperative Nosocomial infections among Patients admitted at Felege Hiwot Referral Hospital, Bahir Dar, Northwest Ethiopia, 2 (6), 140–147. |
| [11] | Mengesha, R. E., Kasa, B. G., Saravanan, M., & Berhe, D. F. (2014). Aerobic bacteria in post surgical wound infections and pattern of their antimicrobial susceptibility in Ayder Teaching and Referral, 4–9. |
| [12] | Akoko, L. O., Mwanga, A. H., Fredrick, F., Mbembati, N. M., & Health, C. (2012). 12 2073 073-, 17 (December), 12–17. |
| [13] | Mawalla, B., Mshana, S. E., Chalya, P. L., Imirzalioglu, C., & Mahalu, W. (2011). Predictors of surgical site infections among patients undergoing major surgery at Bugando Medical Centre in Northwestern Tanzania. BMC Surgery, 11 (1), 21. |
| [14] | Kitembo, S. K., & Chugulu, S. G. (2013). Incidence of Surgical Site Infections and Microbial Pattern at Kilimanjaro Christian Medical Centre. Annals of African Surgery, 10 (1), 27–32. Retrieved from |
| [15] | Mpogoro, F. J., Mshana, S. E., Mirambo, M. M., Kidenya, B. R., & Gumodoka, B. (2014). Incidence and predictors of surgical site infections following caesarean sections at Bugando Medical Centre, Mwanza, Tanzania, 1–10. |
| [16] | Alerany, C., Campany, D., Monterde, J., & Semeraro, C. (2005). Impact of local guidelines and an integrated dispensing system on antibiotic prophylaxis quality in a surgical centre. Journal of Hospital Infection, 60 (2), 111–117. |
| [17] | Allerberger, F., Gareis, R., Jindrák, V., & Struelens, M. J. (2009). Antibiotic stewardship implementation in the EU: the way forward. Expert Review of Anti-Infective Therapy, 7 (10), 1175–1183. |
| [18] | Hawn, M. T., Richman, J. S., Vick, C. C., Deierhoi, R. J., Graham, L. A., Henderson, W. G., & Itani, K. M. F. (2013). Timing of Surgical Antibiotic Prophylaxis and the Risk of Surgical Site Infection. JAMA Surgery, 148 (7), 649. |
| [19] | Gorbach, S. L., Condon, R. E., Conte, J. E., Kaiser, A. B., Ledger, W. J., & Nichols, R. L. (1992). Evaluation of new anti-infective drugs for surgical prophylaxis. Infectious Diseases Society of America and the Food and Drug Administration. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 15 Suppl 1, S313-38. Retrieved from |
| [20] | Anderson, D. J., Podgorny, K., Berríos-Torres, S. I., Bratzler, D. W., Dellinger, E. P., Greene, L.,… Kaye, K. S. (2014). Strategies to Prevent Surgical Site Infections in Acute Care Hospitals: 2014 Update. Infection Control & Hospital Epidemiology, 35 (6), 605–627. |
| [21] | Bratzler, D. W., Dellinger, E. P., Olsen, K. M., Perl, T. M., Auwaerter, P. G., Bolon, M. K.,… Weinstein, R. A. (2013). Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery. Surgical Infections, 14 (1), 73–156. |
| [22] | Steinberg, J. P., Braun, B. I., Hellinger, W. C., Kusek, L., Bozikis, M. R., Bush, A. J.,… Kritchevsky, S. B. (2009). Timing of Antimicrobial Prophylaxis and the Risk of Surgical Site Infections. Annals of Surgery, 250 (1), 10–16. |
| [23] | Weber, W. P., Marti, W. R., Zwahlen, M., Misteli, H., Rosenthal, R., Reck, S.,… Widmer, A. F. (2008). The Timing of Surgical Antimicrobial Prophylaxis. Annals of Surgery, 247 (6), 918–926. |
| [24] | Allegranzi, B., Zayed, B., Bischoff, P., Kubilay, N. Z., de Jonge, S., de Vries, F.,… Solomkin, J. S. (2016). New WHO recommendations on intraoperative and postoperative measures for surgical site infection prevention: an evidence-based global perspective. The Lancet Infectious Diseases, 16 (12), e288–e303. |
| [25] | Nooyen, S. M., Overbeek, B. P., Brutel de la Rivière, A., Storm, A. J., & Langemeyer, J. J. (1994). Prospective randomised comparison of single-dose versus multiple-dose cefuroxime for prophylaxis in coronary artery bypass grafting. European Journal of Clinical Microbiology & Infectious Diseases : Official Publication of the European Society of Clinical Microbiology, 13 (12), 1033–7. Retrieved from |
| [26] | Tamayo, E., Gualis, J., Flórez, S., Castrodeza, J., Eiros Bouza, J. M., & Álvarez, F. J. (2008). Comparative study of single-dose and 24-hour multiple-dose antibiotic prophylaxis for cardiac surgery. The Journal of Thoracic and Cardiovascular Surgery, 136 (6), 1522–1527. |
| [27] | Danda, A. K., Wahab, A., Narayanan, V., & Siddareddi, A. (2010). Single-Dose Versus Single-Day Antibiotic Prophylaxis for Orthognathic Surgery: A Prospective, Randomized, Double-Blind Clinical Study. Journal of Oral and Maxillofacial Surgery, 68 (2), 344–346. |
| [28] | Kang, S.-H., Yoo, J.-H., & Yi, C.-K. (2009). The Efficacy of Postoperative Prophylactic Antibiotics in Orthognathic Surgery: A Prospective Study in Le Fort I Osteotomy and Bilateral Intraoral Vertical Ramus Osteotomy. Yonsei Medical Journal, 50 (1), 55. |
| [29] | Wahab, P. U. A., Narayanan, V., Nathan, S., & Madhulaxmi. (2013). Antibiotic prophylaxis for bilateral sagittal split osteotomies: a randomized, double-blind clinical study. International Journal of Oral and Maxillofacial Surgery, 42 (3), 352–355. |
| [30] | Saxer, F., Widmer, A., Fehr, J., Soka, I., Kibatala, P., Urassa, H.,… Hatz, C. (2009). Benefit of a Single Preoperative Dose of Antibiotics in a Sub-Saharan District Hospital: Minimal Input, Massive Impact. Annals of Surgery, 249 (2), 322–326. |
| [31] | Ondari, J. N., Masika, M. M., Ombachi, R. B., & Ating’a, J. E. (2016). Unblinded randomized control trial on prophylactic antibiotic use in gustilo II open tibia fractures at Kenyatta National Hospital, Kenya. Injury, 47 (10), 2288–2293. |
| [32] | Kusachi, S., Sumiyama, Y., Nagao, J., Arima, Y., Yoshida, Y., Tanaka, H.,… Sato, J. (2008). Prophylactic antibiotics given within 24 hours of surgery, compared with antibiotics given for 72 hours perioperatively, increased the rate of methicillin-resistant Staphylococcus aureus isolated from surgical site infections. Journal of Infection and Chemotherapy, 14 (1), 44–50. |
| [33] | Nguhuni, B., Nardo, P. De, Gentilotti, E., Chaula, Z., Damian, C., Mencarini, P.,… Ippolito, G. (2017). Reliability and validity of using telephone calls for post-discharge surveillance of surgical site infection following caesarean section at a tertiary hospital in Tanzania, 4–9. |
| [34] | Nardo, P. De, Gentilotti, E., Nguhuni, B., Vairo, F., Chaula, Z., Nicastri, E.,… Ippolito, G. (2016). Post-caesarean section surgical site infections at a Tanzanian tertiary Post-caesarean section surgical site infections at a Tanzanian tertiary hospital : a prospective observational study. Journal of Hospital Infection, 93 (4), 355–359. |
| [35] | Fehr, J., Hatz, C., Soka, I., Kibatala, P., Urassa, H., Smith, T.,… Mshinda, H. (2014). Risk Factors for Surgical Site Infection in a Tanzanian District Hospital : A Challenge for the Traditional National Nosocomial Infections Surveillance System Index • Risk Factors for Surgical Site Infection in a Tanzanian District Hospital : A Challenge, (May). |
| [36] | Petrosillo, N., Drapeau, C. M. J., Nicastri, E., Martini, L., Ippolito, G., Moro, M. L., & ANIPIO. (2008). Surgical site infections in Italian Hospitals: a prospective multicenter study. BMC Infectious Diseases, 8, 34. |
| [37] | Fan Y, Wei Z, Wang W, Tan L, Jiang H, Jiang H, Tian L and Nie S (2014). The incidence and distribution of surgical site infection in Mainland China: A meta-analysis of 84 prospective observational studies. Scientific Reports, 4, 1-8. |
| [38] | Laloto, T. L., Gemeda, D. H., & Abdella, S. H. (2017). Incidence and predictors of surgical site infection in Ethiopia : prospective cohort, 1–9. |
| [39] | Taye M. Wound Infection in Tikur Anbessa hospital, surgical department, Ethiop Med J 2005, 43: 167-174. |
| [40] | Yohannes, Y., Mengesha, Y., & Tewelde, Y. (2009). Timing, choice and duration of perioperative prophylactic antibiotic use in surgery : A teaching hospital based experience from Eritrea, in 2009, 65–67. |
| [41] | Dellinger, E. P., Hausmann, S. M., Bratzler, D. W., Johnson, R. M., Daniel, D. M., Bunt, K. M.,… Sugarman, J. R. (2005). Hospitals collaborate to decrease surgical site infections. The American Journal of Surgery, 190 (1), 9–15. |
| [42] | Mbchb, K. J. W. M., Ortho, M., Dip, T. C., & Clinical, O. (2012). Audit of prophylactic antibiotic use in orthopaedic surgery in Mulago Hospital, 9 (January), 16–18. |
| [43] | Bank, N. W. (2014). Adherence to guidelines of antibiotic prophylactic use in surgery : a prospective cohort study in, 1–7. |
| [44] | Shapiro, M. (n.d.). Perioperative prophylactic use of antibiotics in surgery: principles and practice. Infection Control : IC, 3 (1), 38–40. Retrieved from |
| [45] | Argaw, N. A., Shumbash, K. Z., & Asfaw, A. A. (2017). Assessment of surgical antimicrobial prophylaxis in Orthopaedics and Traumatology Surgical Unit of a Tertiary Care Teaching Hospital in Addis Ababa. BMC Research Notes, 6–13. |
| [46] | Mazaki, T., Mado, K., Masuda, H., Shiono, M., Tochikura, N., & Kaburagi, M. (2014). A randomized trial of antibiotic prophylaxis for the prevention of surgical site infection after open mesh-plug hernia repair. The American Journal of Surgery, 207 (4), 476–484. |
| [47] | Mazaki, T., Mado, K., Masuda, H., & Shiono, M. (2013). Antibiotic Prophylaxis for the Prevention of Surgical Site Infection after Tension-Free Hernia Repair: A Bayesian and Frequentist Meta-Analysis. Journal of the American College of Surgeons, 217 (5), 788–801. e4. |
| [48] | Aiken, A. M., Karuri, D. M., Wanyoro, A. K., & Macleod, J. (2012). Interventional studies for preventing surgical site infections in sub-Saharan Africa - A systematic review. International Journal of Surgery, 10 (5), 242–249. |
| [49] | Itani, K. M. (2013). Urological Survey Infection and Inflammation of Genitourinary Tract Re : Timing of Surgical Antibiotic Prophylaxis and the Risk of Surgical Site Re : Urothelial Carcinoma with Prominent Squamous Differentiation in the Diagnostic Urology, Urinary Diversio, 190 (December), 2102–2103. |
| [50] | Chilonga, K. S., Philemon, R. N., Katundu, D., & Lugakingira, A. (2017). Surgical Site Infection : The Rate and Antimicrobial Sensitivity Pattern in Electively Operated Surgical and Gynecological Patients at Kilimanjaro Christian Medical Centre, Northern Tanzania, 3, 1–5. |
APA Style
Kato, P. P., Chotta, N. A. S., Juma, M. A. (2024). Surgical Antibiotic Prophylaxis Practices and Occurrence of Surgical Site Infections Among Operated Patients at Dodoma Regional Referral Hospital, Tanzania . Journal of Surgery, 12(2), 20-32. https://doi.org/10.11648/j.js.20241202.12
ACS Style
Kato, P. P.; Chotta, N. A. S.; Juma, M. A. Surgical Antibiotic Prophylaxis Practices and Occurrence of Surgical Site Infections Among Operated Patients at Dodoma Regional Referral Hospital, Tanzania . J. Surg. 2024, 12(2), 20-32. doi: 10.11648/j.js.20241202.12
AMA Style
Kato PP, Chotta NAS, Juma MA. Surgical Antibiotic Prophylaxis Practices and Occurrence of Surgical Site Infections Among Operated Patients at Dodoma Regional Referral Hospital, Tanzania . J Surg. 2024;12(2):20-32. doi: 10.11648/j.js.20241202.12
@article{10.11648/j.js.20241202.12,
author = {Peleus Peter Kato and Nikolas Albert Sagumo Chotta and Mwinyikondo Amir Juma},
title = {Surgical Antibiotic Prophylaxis Practices and Occurrence of Surgical Site Infections Among Operated Patients at Dodoma Regional Referral Hospital, Tanzania
},
journal = {Journal of Surgery},
volume = {12},
number = {2},
pages = {20-32},
doi = {10.11648/j.js.20241202.12},
url = {https://doi.org/10.11648/j.js.20241202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241202.12},
abstract = {This study was conducted to determine association between perioperative antibiotic prophylaxis practices and occurrence of surgical site infections at Dodoma Regional Referral Hospital in Tanzania. Surgical site infections (SSIs) are preventable complications following surgery, but still cause significant burden in terms of patient morbidity, mortality and increased cost of treatment. A prospective cohort study was conducted among 162 operated patients. Patients with different trends of antibiotic prophylaxis were followed up for occurrence SSIs. Analysis of data was done by SPSS version 20 program using frequency tables, chi square test, Kaplan-meier and Cox regression methods. Significance level of < 0.05 was taken to establish associations between variables. It was found that, 60.5% of patients received preoperative antibiotic prophylaxis, the overall surgical site infections rate was 14.8%. There was no significant difference in occurrence of surgical site infections between patients who received and those who did not receive preoperative antibiotic prophylaxis (p=0.88). The study concluded that SSIs are significant complications. Perioperative antibiotic prophylaxis is commonly practiced. Establishment of local protocol on antibiotic prophylaxis and adherence to infection prevention can improve the prevailing situation.
},
year = {2024}
}
TY - JOUR T1 - Surgical Antibiotic Prophylaxis Practices and Occurrence of Surgical Site Infections Among Operated Patients at Dodoma Regional Referral Hospital, Tanzania AU - Peleus Peter Kato AU - Nikolas Albert Sagumo Chotta AU - Mwinyikondo Amir Juma Y1 - 2024/04/02 PY - 2024 N1 - https://doi.org/10.11648/j.js.20241202.12 DO - 10.11648/j.js.20241202.12 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 20 EP - 32 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20241202.12 AB - This study was conducted to determine association between perioperative antibiotic prophylaxis practices and occurrence of surgical site infections at Dodoma Regional Referral Hospital in Tanzania. Surgical site infections (SSIs) are preventable complications following surgery, but still cause significant burden in terms of patient morbidity, mortality and increased cost of treatment. A prospective cohort study was conducted among 162 operated patients. Patients with different trends of antibiotic prophylaxis were followed up for occurrence SSIs. Analysis of data was done by SPSS version 20 program using frequency tables, chi square test, Kaplan-meier and Cox regression methods. Significance level of < 0.05 was taken to establish associations between variables. It was found that, 60.5% of patients received preoperative antibiotic prophylaxis, the overall surgical site infections rate was 14.8%. There was no significant difference in occurrence of surgical site infections between patients who received and those who did not receive preoperative antibiotic prophylaxis (p=0.88). The study concluded that SSIs are significant complications. Perioperative antibiotic prophylaxis is commonly practiced. Establishment of local protocol on antibiotic prophylaxis and adherence to infection prevention can improve the prevailing situation. VL - 12 IS - 2 ER -
Department of Paediatrics, Dodoma Regional Referral Hospital, Dodoma, Tanzania
Information