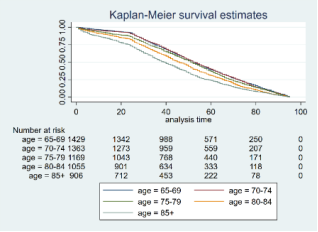
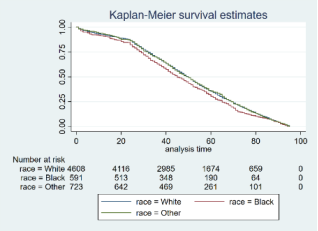
Background: The postoperative survival time and prognosis of elderly patients with colorectal cancer are influenced by numerous factors. This study analyzes these factors to provide references for clinical prognostic evaluation. Methods: Elderly patients who underwent radical surgery for colorectal cancer were selected from the SEER database. Their data were analyzed using the COX proportional hazards model and the Kaplan-Meier method. Results: The study included 6031 patients, among whom 2902 were male (48.12%) and 3129 were female (51.88%). The racial composition included 4694 Whites (77.83%), 603 Blacks (10.00%), and 734 Asians and other races (12.17%). There were 1440 patients aged 65-69 years (23.88%), 1382 aged 70-74 years (22.91%), 1185 aged 75-79 years (19.65%), 1082 aged 80-84 years (17.94%), and 942 aged over 85 years (15.62%). The median survival time for elderly patients who died post-surgery was 49 months, with a 1-year survival rate of 92.42%, a 2-year survival rate of 86.13%, a 3-year survival rate of 68.65%, a 4-year survival rate of 51.27%, and a 5-year survival rate of 34.96%. Univariate analysis indicated that age, race, extent of tumor metastasis, tumor stage, and TNM stage were related factors influencing postoperative prognosis. The COX proportional hazards model analysis showed that age and race were independent risk factors for postoperative prognosis. Patients older than 75 years had a poorer prognosis post-surgery. Among racial groups, Whites had a longer survival period compared to Blacks. Stratified analysis revealed that for patients with local metastasis, both age and race were influential factors for prognosis, while for patients with distant metastasis, age was the influencing factor. Interaction analysis of different factors indicated that patients over 85 years of age who were either Asian or from other races, those over 85 years of age with distant tumor metastasis, and those aged 85 or older with stage IV tumors had a poorer prognosis. Conclusion: Age and race are independent risk factors affecting the postoperative prognosis of elderly colorectal cancer patients. The impact of these factors varies with different levels of tumor metastasis. Thus, understanding the clinical characteristics of elderly colorectal cancer patients can provide evidence for optimizing postoperative treatment and improving prognosis.
| Published in | International Journal of Clinical Oncology and Cancer Research (Volume 10, Issue 2) |
| DOI | 10.11648/j.ijcocr.20251002.17 |
| Page(s) | 99-105 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Colorectal Cancer, Elderly Patients, Radical Surgery, Prognosis Factors, Survival Analysis
Characteristics | N (%) |
|---|---|
Age(years) | |
65-69 | 1440(23.88) |
70-74 | 1382(22.91) |
75-79 | 1185(19.65) |
80-84 | 1082(17.94) |
≥85 | 942(15.62) |
Gender | |
Male | 2902(48.12) |
Female | 3129(51.88) |
Race | |
Whites | 4694(77.83) |
Blacks | 603(10.00) |
Asians and other | 734(12.17) |
Extent of tumor metastasis | |
Local | 5993(99.37) |
Regional | 6(0.10) |
Distant | 32(0.53) |
Tumor stage | |
I | 5990(99.32) |
II | 6(0.10) |
III | 4(0.07) |
IV | 31(0.51) |
T stage | |
T1 | 3115(51.65) |
T2 | 2885(47.84) |
T3 | 15(0.25) |
T4 | 16(0.27) |
N stage | |
N0 | 6003(99.54) |
N1 | 28(0.46) |
M stage | |
M0 | 6000(99.49) |
M1 | 31(0.51) |
Variables | n | χ2 | P |
|---|---|---|---|
Age (years) | 139.47 | <0.001 | |
65-69 | 1440 | ||
70-74 | 1382 | ||
75-79 | 1185 | ||
80-84 | 1082 | ||
≥85 | 942 | ||
Gender | 0.26 | 0.6072 | |
Male | 2902 | ||
Female | 3129 | ||
Race | 9.23 | 0.0099 | |
Whites | 4694 | ||
Blacks | 603 | ||
Asians and other | 734 | ||
Extent of tumor metastasis | 33.93 | <0.001 | |
Local | 5993 | ||
Regional | 6 | ||
Distant | 32 | ||
Tumor stage | 32.15 | <0.001 | |
I | 5990 | ||
II | 6 | ||
III | 4 | ||
IV | 31 | ||
T stage | 34.37 | <0.001 | |
T1 | 3115 | ||
T2 | 2885 | ||
T3 | 15 | ||
T4 | 16 | ||
N stage | 17.65 | <0.001 | |
N0 | 6003 | ||
N1 | 28 | ||
M stage | 30.78 | <0.001 | |
M0 | 6000 | ||
M1 | 31 |
Variables | HR | 95%CI | P |
|---|---|---|---|
Age (years) | |||
65-69 | 1 | ||
70-74 | 1.021 | 0.948-1.100 | 0.585 |
75-79 | 1.092 | 1.010-1.180 | 0.027 |
80-84 | 1.294 | 1.194-1.402 | <0.001 |
≥85 | 1.547 | 1.422-1.684 | <0.001 |
Race | |||
Whites | 1 | ||
Blacks | 1.197 | 1.098-1.305 | <0.001 |
Asians and other | 1.045 | 0.966-1.131 | 0.271 |
Extent of tumor metastasis | 2.141 | 0.636-7.207 | 0.219 |
Tumor stage | 1.000 | 0.402-2.484 | 0.999 |
T stage | 1.018 | 0.967-1.072 | 0.485 |
N stage | 0.648 | 0.271-1.548 | 0.329 |
M stage | 0.941 | 0.254-3.486 | 0.928 |
Variables | Local metastasis | Distant metastasis | ||
|---|---|---|---|---|
HR | P | HR | P | |
Age | 1.110 | <0.001 | 1.730 | 0.010 |
Race | 1.041 | 0.034 | 0.738 | 0.325 |
Variables | HR | 95%CI | P |
|---|---|---|---|
Age # Race | |||
≥85# Asians and other | 1.606 | 1.226-2.104 | 0.001 |
Age#Extent of tumor metastasis | |||
≥85#Distant | 7.286 | 2.270-23.278 | 0.001 |
Age#Tumor stage | |||
≥85# IV | 7.292 | 2.272-23.399 | 0.001 |
IARC | International Agency for Research on Cancer |
SEER | Surveillance, Epidemiology, and End Results |
AJCC | American Joint Committee on Cancer |
HR | Hazard Ratio |
| [1] | Dekker E, Tanis PJ, Vleugels JLA, et al. Colorectal cancer. Lancet. 2019; 394(10207): 1467-1480. |
| [2] | Baidoun F, Elshiwy K, Elkeraie Y, et al. Colorectal CancerEpidemiology: Recent Trends and Impact on Outcomes. Curr Drug Targets. 2021; 22(9): 998-1009. |
| [3] | Klimeck L, Heisser T, Hoffmeister M, et al. Colorectal cancer: A health and economic problem. Best Pract Res Clin Gastroenterol. 2023; 66: 101839. |
| [4] | Shi JF, Wang L, Ran JC, et al. Clinical characteristics, medical service utilization, and expenditure for colorectal cancer in China, 2005 to 2014: Overall design and results froma multicenter retrospective epidemiologic survey. Cancer. 2021; 127(11): 1880-1893. |
| [5] | Lang D, Ciombor KK. Diagnosis and Management of Rectal Cancer in Patients Younger Than 50 Years: Rising Global Incidence and Unique Challenges. J Natl Compr Canc Netw. 2022; 20(10): 1169-1175. |
| [6] | Fan S, Zhao Z, Wang H, et al. Efficacy and safety of oxaliplatin-based chemotherapy as first-line treatment in elderlypatients with metastatic colorectal cancer: a meta-analysis. Front Oncol. 2025; 15: 1567732. Published 2025 Apr 7. |
| [7] | Chen E, Chen L, Zhang W. Robotic-assisted colorectal surgery in colorectal cancer management: a narrative review of clinical efficacy and multidisciplinary integration. Front Oncol. 2025; 15: 1502014. Published 2025 Apr 7. |
| [8] | Wang C, Wang Y, Zhang H, et al. Short-term outcomes of KangDuo surgical robot- versus Da Vinci surgical robot-assisted radical resection of colorectal cancer: a prospective cohort study. BMC Surg. 2025; 25(1): 161. Published 2025 Apr 16. |
| [9] | Abdel Hamid M, Pammer LM, Oberparleiter S, et al. Multidimensional differences of right- and left-sided colorectal cancer and their impact on targeted therapies. NPJ Precis Oncol. 2025; 9(1): 116. Published 2025 Apr 22. |
| [10] | Lu Y, Zhao X, Liu H, Zhang Y, Guo L, Wang L. The prognostic significance of tumor-specific growth factor in colorectal cancer: an observation study. BMC Gastroenterol. 2025; 25(1): 280. Published 2025 Apr 21. |
| [11] | de Wit M, Dekker E, Spaander M, et al. Developing a New Stool Test for Colorectal Cancer Screening, the multitargetFIT (mtFIT). Dig Dis Sci. Published online April 15, 2025. |
| [12] | Xu DG, Tan J. Interplay of genetic and clinical factors in cancer-associated thrombosis: Deciphering the prothrombotic landscape of colorectal cancer. World J Gastroenterol. 2025; 31(14): 103901. |
| [13] | Takagi M, Kim S, Suzuki M, et al.Factors associated with postoperative recurrence in perforated colorectal cancer: unraveling the high recurrence rate of perforated colorectal cancer. World J Surg Oncol. 2025; 23(1): 139. Published 2025 Apr 11. |
| [14] | Wang J, Yang Y, Li W, et al. Application value of laparoscopic surgery in elderly patients (≥ 75 years) with colorectal cancer and prognostic factors influencing 5-year overall survival. Am J Transl Res. 2024; 16(6): 2633-2644. Published 2024 Jun 15. |
| [15] | Liang T, Jiang J, Li X, et al. Preoperative carcinoembryonic antigen to lymphocyte ratio serves as a prognostic predictor in elderly patients with colorectal cancer: a multicentre retrospective study. BMJ Open. 2025; 15(1): e086432. Published 2025 Jan 20. |
| [16] | Samara AA, Diamantis A, Magouliotis D, et al. Assessing Preoperative (EORTC) QLQ-C30 Score in Elderly Patients with Colorectal Cancer: Results from a Prospective Cohort Study. J Clin Med. 2024; 13(20): 6193. Published 2024 Oct 17. |
| [17] | Zhao FQ, Jiang YJ, Xing W, et al. The safety and prognosis of radical surgery in colorectal cancer patients over 80 years old [published correction appears in BMC Surg. 2023 Mar 29; 23(1): 72. BMC Surg. 2023; 23(1): 45. Published 2023 Feb 28. |
| [18] | Devoto L, Celentano V, Cohen R, Khan J, Chand M. Colorectal cancer surgery in the very elderly patient: a systematic review of laparoscopic versus open colorectal resection. Int J Colorectal Dis. 2017; 32(9): 1237-1242. |
| [19] | Losurdo P, Mastronardi M, de Manzini N, Bortul M. Survival and long-term surgical outcomes after colorectal surgery: are there any gender-related differences?. Updates Surg. 2022; 74(4): 1337-1343. |
| [20] | Shalata W, Gluzman A, Man S, et al. Colorectal Cancer in Elderly Patients: Insights into Presentations, Prognosis, and Patient Outcomes. Medicina (Kaunas). 2024; 60(12): 1951. Published 2024 Nov 26. |
| [21] | Micu BV, Vesa ŞC, Pop TR, Micu CM. Evaluation of prognostic factors for 5 year-survival after surgery for colorectal cancer. Ann Ital Chir. 2020; 91: 41-48. PMID: 32180583. |
APA Style
Xu, B., Wang, B., Xiao, Y., Zhang, J., Li, D., et al. (2025). Prognostic Factors and Survival Analysis after Radical Surgery in Elderly Patients with Colorectal Cancer Based on SEER Database. International Journal of Clinical Oncology and Cancer Research, 10(2), 99-105. https://doi.org/10.11648/j.ijcocr.20251002.17
ACS Style
Xu, B.; Wang, B.; Xiao, Y.; Zhang, J.; Li, D., et al. Prognostic Factors and Survival Analysis after Radical Surgery in Elderly Patients with Colorectal Cancer Based on SEER Database. Int. J. Clin. Oncol. Cancer Res. 2025, 10(2), 99-105. doi: 10.11648/j.ijcocr.20251002.17
@article{10.11648/j.ijcocr.20251002.17,
author = {Bingqing Xu and Bing Wang and Yang Xiao and Jianyu Zhang and Daojun Li and Shijun Li and Guoliang Liu and Kezhi Shi},
title = {Prognostic Factors and Survival Analysis after Radical Surgery in Elderly Patients with Colorectal Cancer Based on SEER Database
},
journal = {International Journal of Clinical Oncology and Cancer Research},
volume = {10},
number = {2},
pages = {99-105},
doi = {10.11648/j.ijcocr.20251002.17},
url = {https://doi.org/10.11648/j.ijcocr.20251002.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcocr.20251002.17},
abstract = {Background: The postoperative survival time and prognosis of elderly patients with colorectal cancer are influenced by numerous factors. This study analyzes these factors to provide references for clinical prognostic evaluation. Methods: Elderly patients who underwent radical surgery for colorectal cancer were selected from the SEER database. Their data were analyzed using the COX proportional hazards model and the Kaplan-Meier method. Results: The study included 6031 patients, among whom 2902 were male (48.12%) and 3129 were female (51.88%). The racial composition included 4694 Whites (77.83%), 603 Blacks (10.00%), and 734 Asians and other races (12.17%). There were 1440 patients aged 65-69 years (23.88%), 1382 aged 70-74 years (22.91%), 1185 aged 75-79 years (19.65%), 1082 aged 80-84 years (17.94%), and 942 aged over 85 years (15.62%). The median survival time for elderly patients who died post-surgery was 49 months, with a 1-year survival rate of 92.42%, a 2-year survival rate of 86.13%, a 3-year survival rate of 68.65%, a 4-year survival rate of 51.27%, and a 5-year survival rate of 34.96%. Univariate analysis indicated that age, race, extent of tumor metastasis, tumor stage, and TNM stage were related factors influencing postoperative prognosis. The COX proportional hazards model analysis showed that age and race were independent risk factors for postoperative prognosis. Patients older than 75 years had a poorer prognosis post-surgery. Among racial groups, Whites had a longer survival period compared to Blacks. Stratified analysis revealed that for patients with local metastasis, both age and race were influential factors for prognosis, while for patients with distant metastasis, age was the influencing factor. Interaction analysis of different factors indicated that patients over 85 years of age who were either Asian or from other races, those over 85 years of age with distant tumor metastasis, and those aged 85 or older with stage IV tumors had a poorer prognosis. Conclusion: Age and race are independent risk factors affecting the postoperative prognosis of elderly colorectal cancer patients. The impact of these factors varies with different levels of tumor metastasis. Thus, understanding the clinical characteristics of elderly colorectal cancer patients can provide evidence for optimizing postoperative treatment and improving prognosis.
},
year = {2025}
}
TY - JOUR T1 - Prognostic Factors and Survival Analysis after Radical Surgery in Elderly Patients with Colorectal Cancer Based on SEER Database AU - Bingqing Xu AU - Bing Wang AU - Yang Xiao AU - Jianyu Zhang AU - Daojun Li AU - Shijun Li AU - Guoliang Liu AU - Kezhi Shi Y1 - 2025/06/06 PY - 2025 N1 - https://doi.org/10.11648/j.ijcocr.20251002.17 DO - 10.11648/j.ijcocr.20251002.17 T2 - International Journal of Clinical Oncology and Cancer Research JF - International Journal of Clinical Oncology and Cancer Research JO - International Journal of Clinical Oncology and Cancer Research SP - 99 EP - 105 PB - Science Publishing Group SN - 2578-9511 UR - https://doi.org/10.11648/j.ijcocr.20251002.17 AB - Background: The postoperative survival time and prognosis of elderly patients with colorectal cancer are influenced by numerous factors. This study analyzes these factors to provide references for clinical prognostic evaluation. Methods: Elderly patients who underwent radical surgery for colorectal cancer were selected from the SEER database. Their data were analyzed using the COX proportional hazards model and the Kaplan-Meier method. Results: The study included 6031 patients, among whom 2902 were male (48.12%) and 3129 were female (51.88%). The racial composition included 4694 Whites (77.83%), 603 Blacks (10.00%), and 734 Asians and other races (12.17%). There were 1440 patients aged 65-69 years (23.88%), 1382 aged 70-74 years (22.91%), 1185 aged 75-79 years (19.65%), 1082 aged 80-84 years (17.94%), and 942 aged over 85 years (15.62%). The median survival time for elderly patients who died post-surgery was 49 months, with a 1-year survival rate of 92.42%, a 2-year survival rate of 86.13%, a 3-year survival rate of 68.65%, a 4-year survival rate of 51.27%, and a 5-year survival rate of 34.96%. Univariate analysis indicated that age, race, extent of tumor metastasis, tumor stage, and TNM stage were related factors influencing postoperative prognosis. The COX proportional hazards model analysis showed that age and race were independent risk factors for postoperative prognosis. Patients older than 75 years had a poorer prognosis post-surgery. Among racial groups, Whites had a longer survival period compared to Blacks. Stratified analysis revealed that for patients with local metastasis, both age and race were influential factors for prognosis, while for patients with distant metastasis, age was the influencing factor. Interaction analysis of different factors indicated that patients over 85 years of age who were either Asian or from other races, those over 85 years of age with distant tumor metastasis, and those aged 85 or older with stage IV tumors had a poorer prognosis. Conclusion: Age and race are independent risk factors affecting the postoperative prognosis of elderly colorectal cancer patients. The impact of these factors varies with different levels of tumor metastasis. Thus, understanding the clinical characteristics of elderly colorectal cancer patients can provide evidence for optimizing postoperative treatment and improving prognosis. VL - 10 IS - 2 ER -
Department of Oncology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Department of Anesthesiology, Yichang Central People's Hospital & The First College of Clinical Medical Science of Three Gorges University, Yichang, China
Information