Purpose: evaluating relationship between serum level of TSH Receptor Antibody (TRAb) and severity of Graves’ ophthalmopathy (GO). Methods: prospective interventional follow up study included 35 newly diagnosed untreated patients with GO was carried at Ain Shams University Hospital, Cairo. patients were subjected to full ophthalmological examination, measuring proptosis degree by Hertel’s Exophthalmometer, measuring TRAb serum level. patients were classified according to clinical activity score into 2 groups: Inactive [CAS < 3]: 23 patients received only antithyroid therapy and Active [CAS ≥ 3]: 12 patients received intravenous methylprednisolone at a dose of 0.5gm for 6 weeks, injected weekly. 6 weeks after treatment severity of (GO), proptosis, and TRAb serum level were reassessed. Results: study found the mean CAS was 2.11±1.13, the mean proptosis measured (23.26 ±3.19) and (22.42 ± 3.27) in right and left eye respectively while mean of TRAb was 11.19 ±6.45. After 6 weeks of treatment, CAS was regressed significantly in relation to TRAb level as TRAb measurement decreased by -62.7%, -14.06% in group II and group I respectively while proptosis measurement of right and left eyes in group II significantly decreased, with mean changes of -10.3% and -10.7%, respectively. And, in group I (-4.5% and -3.8%) in right and left eyes respectively, but not significant to TRAb level. Conclusion TRAb level can be used as monitor to activity of Grave’s Ophthalmopathy (GO) and in follow up but not directly related to proptosis degree.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Graves’ disease (GD) is the most common cause of hyperthyroidism in developed Countries. GD is characterized by hyperthyroidism, diffuse goiter, ophthalmopathy, and dermopathy, In addition to elevated free thyroid hormones and suppressed thyroid stimulating hormone (TSH) levels. It is more common between 30-60 years, 5-10 times more frequent in females
[1]
Antonelli A, Ferrari SM, Ragusa F, Elia G, Paparo SR, Ruffilli I, et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best practice & research. Clinical endocrinology & metabolism. 2020; 34(1).
[1]
.
Grave’s Ophthalmopathy (GO) is an autoimmune inflammation of the orbital tissues and the most common extra-thyroid symptom of GD, that occurs in 25-50% of patients with GD
[2]
Oh S-R, Tung JD, Priel A, Levi L, Granet DB, Korn BS, et al. Reduction of orbital inflammation following decompression for thyroid-related orbitopathy. Biomed Res Int [Internet]. 2013; 2013: 794984. Available from:
The main clinical manifestations of the disease are periorbital edema, eyelid retraction, proptosis, restrictive myopathy, and optic neuropathy. Changes in appearance and exposure symptoms and signs are the most common initial findings in GO. Proptosis is the second most common finding in GO that may be asymmetric and results from inflammation and increased volume of orbital soft tissues, including the extraocular muscles
[3]
Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA, et al. Clinical features of Graves’ ophthalmopathy in an incidence cohort. Am J Ophthalmol [Internet]. 1996; 121(3): 284-90. Available from:
The diagnosis is usually made clinically based on presenting ocular symptoms and signs. Abnormalities in thyroid hormonal tests (free triiodothyronine (T3), free thyroxine (T4), and TSH) and/or the presence of thyroid specific antibodies (anti-thyroglobulin, anti-thyroid peroxidase and (TRAb)) help to support the diagnosis, but sometimes it may be negative especially in late disease
[4]
Diana T, Ponto KA, Kahaly GJ. Correction to: Thyrotropin receptor antibodies and Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2022; 45(1): 233. Available from:
The close link of GO with GD underpin the hypothesis that GO is triggered by immune reactions against one or more antigens shared by thyroid and orbit. Several potential serum markers for GO disease activity have been studied with the hope of monitoring change in activity more accurately. These include urine and serum Glycosaminoglycans (GAGs) and TRAbs
[5]
Nicolì F, Lanzolla G, Mantuano M, Ionni I, Mazzi B, Leo M, et al. Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2021; 44(3): 581-5. Available from:
The onset of GO is usually closely related to GD in its pathognomonic hyperthyroidism phase. Orbitopathy most often develops synchronously, it can also precede or follow the occurrence of hyperthyroidism
[6]
Gontarz-Nowak K, Szychlińska M, Matuszewski W, Stefanowicz-Rutkowska M, Bandurska-Stankiewicz E. Current knowledge on Graves’ orbitopathy. J Clin Med [Internet]. 2020; 10(1): 16. Available from:
. Thyroid stimulating hormone receptor (TSHR), present on the thyroid cells, and physiologically found on the surface of orbital fibroblasts, yet in the case of GO, it is overexpressed
[7]
Bartalena L. Graves’ orbitopathy: imperfect treatments for a rare disease. Eur Thyroid J [Internet]. 2013; 2(4): 259-69. Available from:
Recent research suggests that onset of orbital inflammation may be characterized by early infiltration of macrophage cells in the orbital region, which induce TSHR antibodies (TRAbs) followed by a subsequent infiltration of CD8+-specific T-cells and fibrocyte
[8]
Philipp, S.; Horstmann, M.; Hose, M.; Daser, A.; Görtz, G. E.; Jesenek, C.; Flögel, U.; Hansen, W.; Bechrakis, N.; Banga, J. P. S.; et al. An Early Wave of Macrophage Infiltration Intertwined with Antigen-Specific Proinflammatory T Cells and Browning of Adipose Tissue Characterizes the Onset of Orbital Inflammation in a Mouse Model of Graves’ Orbitopathy. Thyroid 2022, 32, 283-293. [Google Scholar] [CrossRef].
[8]
. Activation and binding of autoantibodies to the thyrotropin receptors (TSHR) expressed on the surface of orbital fibroblasts that induce proliferation, excess adipogenesis and overproduction of the extracellular matrix. The extracellular matrix comprises glycosaminoglycans (GAGs), such as chondroitin sulfate and hyaluronan. causing local water retention and swelling of connective tissue and extraocular muscles, which in turn worsens the venous and lymphatic circulation in the orbit
[8]
Philipp, S.; Horstmann, M.; Hose, M.; Daser, A.; Görtz, G. E.; Jesenek, C.; Flögel, U.; Hansen, W.; Bechrakis, N.; Banga, J. P. S.; et al. An Early Wave of Macrophage Infiltration Intertwined with Antigen-Specific Proinflammatory T Cells and Browning of Adipose Tissue Characterizes the Onset of Orbital Inflammation in a Mouse Model of Graves’ Orbitopathy. Thyroid 2022, 32, 283-293. [Google Scholar] [CrossRef].
[8]
.
The disease follows a biphasic course with an active or progressive phase followed by a quiescent or stable phase: the temporal status is graded as disease activity. Grading systems for GO include Werner’s NO SPECS and European Group on Graves’ Orbitopathy (EUGOGO)’s severity scales, the Clinical Activity Score (CAS) and the VISA Classification (for severity and activity). Diagnosis of GO is based on recognition of clinical features and supported by thyroid function and immune testing, and orbital imaging
[1]
Antonelli A, Ferrari SM, Ragusa F, Elia G, Paparo SR, Ruffilli I, et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best practice & research. Clinical endocrinology & metabolism. 2020; 34(1).
[1]
.
Early diagnosis of GO allows appropriate evaluation and treatment, and ideally might prevent the development of more serious sequalae. The endocrinologist or internist can play a vital role in recognizing early ocular clinical manifestations, determining disease severity and activity, identifying those most at risk for developing serious complications, and in arranging prompt referral to an experienced ophthalmologist so that appropriate intervention can be planned
[4]
Diana T, Ponto KA, Kahaly GJ. Correction to: Thyrotropin receptor antibodies and Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2022; 45(1): 233. Available from:
. Our study aims to evaluate the relationship between serum level of TSH receptor antibody (TRab) and severity of Grave’s ophthalmopathy in order to help early diagnosis and treatment of the disease to prevent the development of complications.
The management of GO depends on the disease severity and activity. However, the guidelines emphasize the importance of individualizing the treatment strategy, so that potential benefits do not outweigh the possible side effects. It is recommended in routine clinical practice that the quality of life of the patients is estimated based on the use of a validated GO-specific quality of life tool (GO-QoL)
[9]
Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, et al. The 2016 European thyroid association/European group on Graves’ orbitopathy guidelines for the management of Graves’ orbitopathy. Eur Thyroid J [Internet]. 2016; 5(1): 9-26. Available from:
A prospective interventional follow up study was carried at Ain Shams University Hospital, Cairo, Egypt from January 2022 to August 2023 and included 35 (newly diagnosed patients with GO) in accordance with the ethical standards stated by the Ethical Committee of Ain Shams University. Patients who visited the outpatient department of Endocrinology and department of Ophthalmology in El Demerdash Hospitals and newly clinically diagnosed with GO and not received any treatment before were included in the study. While patients with history of previous orbital surgery, thyroid surgery, other autoimmune diseases, and history of previous antithyroid treatment were excluded from the study. All patients were subjected: History taking including name, age and medical history, full ophthalmological examination including detection and measurement of proptosis using Hertel’s exophthalmometer, classification of the patients according to CAS, measurement of serum thyroid profile, measurement of serum level of TRAb by Enzyme-Linked Immunosorbent Assay (ELISA): (Cobas e 801 analyzers, Roche Diagnostics, Mannheim, Germany), remeasurement of the degree of the proptosis and serum level of TRAb after 6 weeks of the treatment.
GO was classified according to history, proptosis (Hertel’s measurement > 17mm or 2 mm differences between the eyes), eyelid retraction (>1 mm in primary gaze), optic neuropathy, ocular motility, corneal or conjunctival involvement. Grading of proptosis severity was done according to the modified NOSPECS score (proptosis <17 mm (0), proptosis 18-19 mm (1), proptosis 20-22 mm (2), proptosis >23 mm (3)).
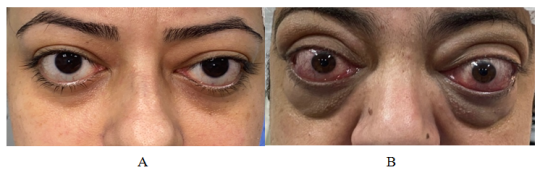
All the GO patients underwent blood tests for surveying the titers of TRAb by Enzyme -linked immunosorbent (ELISA) as well as the concentrations of TSH, FT3 and FT4; moreover, CAS examinations were also performed for evaluating the activity of GO among the patients according to seven assessment items: spontaneous retrobulbar pain, pain on eye movement, eyelid erythema, conjunctival injection, chemosis, swelling of the lacrimal caruncle, and eyelid edema or fullness, One point was given for each item and it ranges from 0-7 scores in total. GO patients were classified according to CAS into 2 groups: inactive group (CAS<3) (n=23) and active group (CAS ≥ 3) (n=12) (Figure 1).
Figure 1. A- patient with inactive GO group I, B- patient with active GO group II.
Inactive patients received only antithyroid treatment, however active patients received antithyroid treatment and intravenous methylprednisolone (IVMP) injected weekly for 6 weeks on the same day at a dose of 0.5 gm. After 6 weeks of treatment, we remeasured proptosis, serum level of TRAb, FT3 and FT4.
3. Statistical Analysis
Data were collected, revised, coded and entered to the Statistical Package for Social Science (IBM SPSS) version 23. The quantitative data were presented as mean, standard deviations and ranges when parametric and median, inter-quartile range (IQR) when data found non-parametric. Also, qualitative variables were presented as number and percentages. The p-value was considered significant as the following: P-value > 0.05: Non-significant (NS), P-value ≤ 0.05: Significant (S), P-value < 0.01: Highly significant (HS).
4. Ethical Considerations
After Approval of the Research Ethical Committee (REC) at the faculty of medicine, Ain Shams University (under the number code FWA 000017585 FAMSU MD 239/2021 and administrative approval was obtained from the manager of Ain Shams University hospitals to carry out the study. A verbal Informed consent was taken from each participant before examination. Confidentiality and privacy of the participants was assured, collected data was dealt in complete confidentiality and used for research purposes.
5. Results
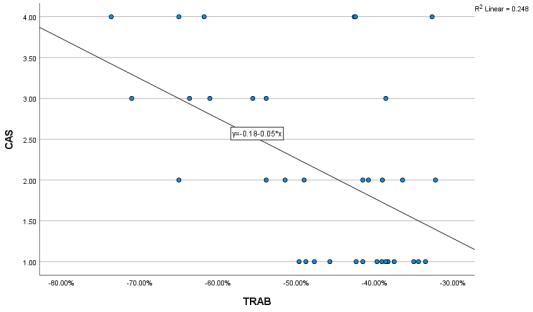
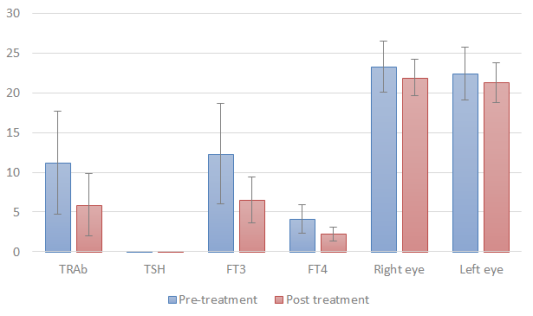
The study included a total of 35 patients ranged from (18-60) years old with mean + SD 33.97±9.48 years, most of the participants were females (62.9%), non-smoker (80%), non-hypertensive (60%), and non-diabetic (54.3%). All patient before treatment were taken all biochemical parameters [Table 1] as The mean CAS was 2.11±1.13, proptosis in 48.6% of the right eye and 40% of the left eye measuring greater than or equal to 23 mm and the mean TRAb 11.19 ±6.45. There is a significant correlation between CAS and proptosis [Table 2] and a significant correlation between TRAb and CAS [Table 3] [Figure 2] while TRAb and proptosis non-significant. The thyroid parameters are non-significant with CAS but TRAb is significant with TSH [Tables 2, 3]. All patients received antithyroid treatment while group 11 received also steroid treatment and mean TRAb 9 (4.2 ± 11) in group I and 5.3 (2.8 ±7.07) in group II in comparison to results before treatment there was a significant drop in the TRAb measurement in the inactive group by -14.06% (-25% - -8.33%) and in the active group by -62.7% (-65.69% - -54.27%) while TSH, FT3, and FT4 significant different before and after the treatment [table 4]. Also, the proptosis measurement of the right and left eyes in active group have significantly decreased, with mean changes of -10.3% (-11.1% - 8%) and -10.7% (-11.1% - -7.4%), respectively. On the other hand, the right and left eyes in the inactive group changed by -4.5% (-4.8% - 0%) and -3.8% (-4.8% - 0%), respectively [Table 4] [Figure 2]. The multiple linear regression analysis was used to evaluate the factors associated with TRAb after treatment [Table 5].
Table 1. Basic characteristics and biochemical parameters before treatment.
Variables
Mean± SD
Range
b (IU/L)
11.19 ±6.45
(1.99 - 27)
TSH (μIU/ml)
0.008±0.003
(0.01 -0.02)
FT3 (pg/dL)
12.31 ±6.30
(4.5 - 25)
FT4 (ng/dL)
4.08 ±1.79
(1.88 -8.53)
CAS
2.11± 1.13
(1-4)
Proptosis
Right eye
23.26 ±3.19
(19 - 30)
Grade 1: 18-19 mm
5.7%
Grade 2: 20-22 mm
45.7%
Grade 3: > 23 mm
48.6%
Left eye
22.42 ± 3.27
(18 - 29)
Grade 1: 18-19 mm
22.9%
Grade 2: 20-22 mm
37.1%
Grade 3: > 23 mm
40.0%
(*) P value ≤0.05 is considered statistically significant ¥independent t test
Table 2. Correlation between CAS and thyroid related parameters and proptosis before treatment.
Parameter
R
P value
Sig.
Right eye proptosis
0.374
0.027
S
Left eye proptosis
0.439
0.008
S
TSH
0.033
0.852
NS
FT3
-0.272
0.115
NS
FT4
-0.257
0.136
NS
(*) P value ≤0.05 is considered statistically significant ¥ spearman’s correlations
Table 3. Correlations between TRAb and thyroid-related parameters, proptosis and CAS before treatment.
Parameters
R
P value
Sig
TSH
-0.501
0.002*
S
FT3
0.190
0.274
NS
FT4
0.235
0.174
NS
Right eye
0.164
0.346
NS
Left eye
0.188
0.279
NS
CAS
-0.498
0.002*
S
(*) P value ≤0.05 is considered statistically significant ¥ pearson correlation was used
Table 4. Biochemical parameters before and after treatment.
Inactive # n=23
Active # n=12
Median (IQR)
Median (IQR)
TRAb before treatment
10 (5.3 - 14)
14.7 (6.4 - 21.15)
TRAb after treatment
9 (4.2 - 11)
5.3 (2.8 - 7.07)
TRAb Change (%)
-14.06% (-25% - -8.33%)
-62.7% (-65.69% - -54.27%)
P-Value
<0.001*
0.002*
TSH before treatment
0.01 (0.005 - 0.01)
0.005 (0.005 - 0.01)
TSH after treatment
0.01 (0.005 - 0.01)
0.01 (0.01 - 0.01)
P-Value
0.059
0.014*
FT3 before treatment
14.5 (9.19 - 19.5)
5.82 (5.12 - 8)
FT3 after treatment
7.9 (5.81 - 9.9)
3.16 (2.5 - 3.9)
P-Value
<0.001*
0.005*
FT4 before treatment
4.8 (2.91 - 5.69)
2.68 (2.2 - 2.8)
FT4 after treatment
2.2 (2 - 3.1)
1.3 (1.3 - 1.4)
P-Value
<0.001*
0.005*
Proptosis Rt eye (mm) before treatment
21 (20 - 23)
27.5 (25 - 29)
Rt eye (mm) after treatment
21 (20 - 22)
24.5 (23 - 26)
Change (%)
-4.5% (-4.8% - 0%)
-10.3% (-11.1% - -8%)
P-Value
<0.001*
0.004*
Lt eye (mm) before treatment
21 (19 - 22)
27 (26 - 27)
Lt eye (mm) after treatment
20 (19 - 22)
24 (23 - 25)
Change (%)
-3.8% (-4.8% - 0%)
-10.7% (-11.1% - -7.4%)
P-Value
<0.001*
0.004*
(*) P value ≤0.05 is considered statistically significant ¥independent t test
Table 5. Multiple linear regression between TRAb and thyroid related parameters and CAS after treatment.
Unstandardized Coefficients
Standardized Coefficients
T
P value
Sig
B
Std. Error
Beta
(Constant)
-0.378
2.982
-0.127
0.90
NS
TSH
64.153
119.566
0.084
0.537
0.59
NS
FT3
0.981
0.321
0.737
3.053
0.10
NS
FT4
-1.247
1.152
-0.275
-1.083
0.28
NS
CAS
1.023
0.618
0.293
1.655
0.01
S
(*) P value ≤0.05 is considered statistically significant ¥independent t test
Figure 3. Comparison between measurements before and after treatment. (Steroid group).
6. Discussion
Graves’ orbitopathy (GO) is a common complication that is clinically relevant in about 50% of patients with GD. The symptoms are often mild, but severe forms of GO occur in 3-5% of patients
[10]
Wiersinga WM, Bartalena L. Epidemiology and prevention of Graves’ ophthalmopathy. Thyroid 2002; 12: 855-860.
. and the GO is the primary cause of exophthalmos in adults as it appears in 30 to 50% of patients with Graves’ disease. About 5% are moderate-to-severe cases that might be see-threatening or lead to long-term disabling sequela. GO may start early in the course of disease or appears later during the follow-up period. In the Middle East, the prevalence of TED among patients with GD is 48% (CI: 0.19 to 0.78) and in Southeast Asia, 35% (CI: 0.24 to 0.47). Regions with a predominance of Caucasians (37%; CI: 0.28 to 0.46) have a lower prevalence of TED than Asian regions (45%; CI: 0.33 to 0.58)
[11]
Chin YH, Ng CH, Lee MH, Koh JWH, Kiew J, Yang SP, et al. Prevalence of thyroid eye disease in Graves’ disease: A meta-analysis and systematic review. Clin Endocrinol (Oxf) [Internet]. 2020; 93(4): 363-74. Available from:
Several studies support the involvement of TRAb in the pathogenesis of GO, and a correlation between GO features and TRAb has been reported, but not confirmed by all studies specially in the initial phase of disease. So, we conducted a follow up interventional study to determine whether there is a correlation between TRAb, CAS and proptosis measurement in the initial phase of the eye disease. In our study we measure of TRAb level by Enzyme -linked immunosorbent (ELISA) which the sensitivity and specificity of TRAb assay are relatively comparable, ranging from 79.5 to 94.4% and 87.5 to 97.9%, respectively
[12]
Struja T, Jutzi R, Imahorn N, et al. Comparison of five TSH‐receptor antibody assays in Graves’ disease: results from an observational pilot study. BMC Endocr Disord. 2019; 19(1): 38.
The correlation between CAS and TRAb level was significant in all patients whose diagnosed GD with GO without initial treatment in our study and this matching with results of Moledina et al
[13]
Moledina M, Roos J, Murthy R. ‘Thyrotropin Receptor Autoantibody Assessment in Thyroid Eye Disease: Does the Assay Type Matter? Korean Journal of Ophthalmology. 2023; 37(2): 147-56.
[13]
and Nicolì et al.
[5]
Nicolì F, Lanzolla G, Mantuano M, Ionni I, Mazzi B, Leo M, et al. Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2021; 44(3): 581-5. Available from:
also TRAb level is significant correlation between with TSH level before treatment, similar to the results of Lin et al
[14]
Lin C-C, Chiu L-W, Lee P-Y, Chen K-J, Cheng K-C. Comparison of the correlation between serum autoantibodies against aldehyde dehydrogenase 2 and thyrotropin receptor in patients with Graves’ ophthalmopathy. Indian J Ophthalmol [Internet]. 2024; 72(2): 298-9. Available from:
. Our study’s the correlation analysis between CAS and thyroid-related parameters (TSH, FT3, and FT4) showed no significant correlation between CAS and thyroid hormones as Similar results to a study by Topcu et al
[15]
Topcu H, Atik BK, Ozkocak BY, Efe AC, Ulas MG, Cabuk KS. Evaluation of aqueous flare in Graves’ ophthalmopathy and its relationship with thyroid hormones, antibodies, and clinical activity score. Beyoglu Eye J [Internet]. 2023; 8(3): 208-13. Available from:
this means that more hormonal changes not actually more clinical activity but more changes of the immunity to TSR.
CAS is a significant correlation with proptosis but the severity of proptosis not related to TRAb level and this is matching with other studies by Nicolì et al.
[5]
Nicolì F, Lanzolla G, Mantuano M, Ionni I, Mazzi B, Leo M, et al. Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2021; 44(3): 581-5. Available from:
Lin C-C, Chiu L-W, Lee P-Y, Chen K-J, Cheng K-C. Comparison of the correlation between serum autoantibodies against aldehyde dehydrogenase 2 and thyrotropin receptor in patients with Graves’ ophthalmopathy. Indian J Ophthalmol [Internet]. 2024; 72(2): 298-9. Available from:
, also after treatment the TRAb level, CAS and Proptosis is improved and decreased as matching with Zang et al
[16]
Zang S, Ponto KA, Pitz S, Kahaly GJ. Dose of intravenous steroids and therapy outcome in Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2011; 34(11): 876-80. Available from:
, which reported a minimum 2-mm reduction in proptosis after IVMP therapy but in our study proptosis in group 11 was decrease larger, at least 3mm while TRAb level in the group 11 that took steroids by -62.7% and in the group 1 by -14.06% (-25% - -8.33%), in line with the findings of Kahaly et al.
[17]
Kahaly GJ, Olivo PD. Graves’ disease. N Engl J Med [Internet]. 2017; 376(2): 184. Available from:
that the TRAb titer significantly decreased following IVMP therapy. The treatment by antithyroid drugs to well control of thyroid function well helping to decrease the stimulus of the immune cascade as the accumulation and overproduction of the extracellular matrix which TRAb will stope stimulating the orbital fibroblast and also the treatment by steroid exaggerate the effect on the TRAb and the infiltration of the activated B and T lymphocytes, as well as bone marrow derived CD34 + and fibrocytes in tissues will stopped this is may be the explanation of the improvement in CAS and proptosis in group 11, further studies for pathophysiology in the future my helping in the management, so TRAb level by ELISA is monitoring for activity of GO in initial diagnosis and after beginning of treatment more less with TSH level for a well control of orbital tissue activity.
7. Conclusion
There has been a significant correlation between the clinical activity of GO and the serum levels of TRAb in patients with a recent-onset, untreated GO as the TRAb level with ELIZA can used as monitoring tool in early diagnosis and in follow-up during treatment for the orbital tissue activity.
8. Limitations of the Study
Small number of cases, Further investigations may be required for more accurate correlation between degree of proptosis and TRab.
Abbreviations
TRAb
Thyroid Receptor Antibody
CAS
Clinical Activity Score
GO
Grave’s Ophhalmopathy
GD
Grave’s Disease
TED
Thyroid Eye Disease
GAGs
Glycosaminoglycans
EUGOGO
Eutopean Group on Grave’s Orbitopathy
TSHR
Thyroid Stimulating Hormone Receptor
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Antonelli A, Ferrari SM, Ragusa F, Elia G, Paparo SR, Ruffilli I, et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best practice & research. Clinical endocrinology & metabolism. 2020; 34(1).
[2]
Oh S-R, Tung JD, Priel A, Levi L, Granet DB, Korn BS, et al. Reduction of orbital inflammation following decompression for thyroid-related orbitopathy. Biomed Res Int [Internet]. 2013; 2013: 794984. Available from:
Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA, et al. Clinical features of Graves’ ophthalmopathy in an incidence cohort. Am J Ophthalmol [Internet]. 1996; 121(3): 284-90. Available from:
Diana T, Ponto KA, Kahaly GJ. Correction to: Thyrotropin receptor antibodies and Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2022; 45(1): 233. Available from:
Nicolì F, Lanzolla G, Mantuano M, Ionni I, Mazzi B, Leo M, et al. Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2021; 44(3): 581-5. Available from:
Gontarz-Nowak K, Szychlińska M, Matuszewski W, Stefanowicz-Rutkowska M, Bandurska-Stankiewicz E. Current knowledge on Graves’ orbitopathy. J Clin Med [Internet]. 2020; 10(1): 16. Available from:
Philipp, S.; Horstmann, M.; Hose, M.; Daser, A.; Görtz, G. E.; Jesenek, C.; Flögel, U.; Hansen, W.; Bechrakis, N.; Banga, J. P. S.; et al. An Early Wave of Macrophage Infiltration Intertwined with Antigen-Specific Proinflammatory T Cells and Browning of Adipose Tissue Characterizes the Onset of Orbital Inflammation in a Mouse Model of Graves’ Orbitopathy. Thyroid 2022, 32, 283-293. [Google Scholar] [CrossRef].
[9]
Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, Marcocci C, et al. The 2016 European thyroid association/European group on Graves’ orbitopathy guidelines for the management of Graves’ orbitopathy. Eur Thyroid J [Internet]. 2016; 5(1): 9-26. Available from:
Chin YH, Ng CH, Lee MH, Koh JWH, Kiew J, Yang SP, et al. Prevalence of thyroid eye disease in Graves’ disease: A meta-analysis and systematic review. Clin Endocrinol (Oxf) [Internet]. 2020; 93(4): 363-74. Available from:
Struja T, Jutzi R, Imahorn N, et al. Comparison of five TSH‐receptor antibody assays in Graves’ disease: results from an observational pilot study. BMC Endocr Disord. 2019; 19(1): 38.
Moledina M, Roos J, Murthy R. ‘Thyrotropin Receptor Autoantibody Assessment in Thyroid Eye Disease: Does the Assay Type Matter? Korean Journal of Ophthalmology. 2023; 37(2): 147-56.
[14]
Lin C-C, Chiu L-W, Lee P-Y, Chen K-J, Cheng K-C. Comparison of the correlation between serum autoantibodies against aldehyde dehydrogenase 2 and thyrotropin receptor in patients with Graves’ ophthalmopathy. Indian J Ophthalmol [Internet]. 2024; 72(2): 298-9. Available from:
Topcu H, Atik BK, Ozkocak BY, Efe AC, Ulas MG, Cabuk KS. Evaluation of aqueous flare in Graves’ ophthalmopathy and its relationship with thyroid hormones, antibodies, and clinical activity score. Beyoglu Eye J [Internet]. 2023; 8(3): 208-13. Available from:
Zang S, Ponto KA, Pitz S, Kahaly GJ. Dose of intravenous steroids and therapy outcome in Graves’ orbitopathy. J Endocrinol Invest [Internet]. 2011; 34(11): 876-80. Available from:
Abbas, K. N. E. D., Elwan, S., Elsherif, R., Nesim, M., Elsamkary, M. (2025). Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. International Journal of Ophthalmology & Visual Science, 10(3), 42-49. https://doi.org/10.11648/j.ijovs.20251003.11
Abbas, K. N. E. D.; Elwan, S.; Elsherif, R.; Nesim, M.; Elsamkary, M. Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. Int. J. Ophthalmol. Vis. Sci.2025, 10(3), 42-49. doi: 10.11648/j.ijovs.20251003.11
Abbas KNED, Elwan S, Elsherif R, Nesim M, Elsamkary M. Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. Int J Ophthalmol Vis Sci. 2025;10(3):42-49. doi: 10.11648/j.ijovs.20251003.11
@article{10.11648/j.ijovs.20251003.11,
author = {Karim Nasr El Din Abbas and Sheriff Elwan and Radwa Elsherif and Mina Nesim and Mahmoud Elsamkary},
title = {Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {10},
number = {3},
pages = {42-49},
doi = {10.11648/j.ijovs.20251003.11},
url = {https://doi.org/10.11648/j.ijovs.20251003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20251003.11},
abstract = {Purpose: evaluating relationship between serum level of TSH Receptor Antibody (TRAb) and severity of Graves’ ophthalmopathy (GO). Methods: prospective interventional follow up study included 35 newly diagnosed untreated patients with GO was carried at Ain Shams University Hospital, Cairo. patients were subjected to full ophthalmological examination, measuring proptosis degree by Hertel’s Exophthalmometer, measuring TRAb serum level. patients were classified according to clinical activity score into 2 groups: Inactive [CAS < 3]: 23 patients received only antithyroid therapy and Active [CAS ≥ 3]: 12 patients received intravenous methylprednisolone at a dose of 0.5gm for 6 weeks, injected weekly. 6 weeks after treatment severity of (GO), proptosis, and TRAb serum level were reassessed. Results: study found the mean CAS was 2.11±1.13, the mean proptosis measured (23.26 ±3.19) and (22.42 ± 3.27) in right and left eye respectively while mean of TRAb was 11.19 ±6.45. After 6 weeks of treatment, CAS was regressed significantly in relation to TRAb level as TRAb measurement decreased by -62.7%, -14.06% in group II and group I respectively while proptosis measurement of right and left eyes in group II significantly decreased, with mean changes of -10.3% and -10.7%, respectively. And, in group I (-4.5% and -3.8%) in right and left eyes respectively, but not significant to TRAb level. Conclusion TRAb level can be used as monitor to activity of Grave’s Ophthalmopathy (GO) and in follow up but not directly related to proptosis degree.},
year = {2025}
}
TY - JOUR
T1 - Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy
AU - Karim Nasr El Din Abbas
AU - Sheriff Elwan
AU - Radwa Elsherif
AU - Mina Nesim
AU - Mahmoud Elsamkary
Y1 - 2025/07/21
PY - 2025
N1 - https://doi.org/10.11648/j.ijovs.20251003.11
DO - 10.11648/j.ijovs.20251003.11
T2 - International Journal of Ophthalmology & Visual Science
JF - International Journal of Ophthalmology & Visual Science
JO - International Journal of Ophthalmology & Visual Science
SP - 42
EP - 49
PB - Science Publishing Group
SN - 2637-3858
UR - https://doi.org/10.11648/j.ijovs.20251003.11
AB - Purpose: evaluating relationship between serum level of TSH Receptor Antibody (TRAb) and severity of Graves’ ophthalmopathy (GO). Methods: prospective interventional follow up study included 35 newly diagnosed untreated patients with GO was carried at Ain Shams University Hospital, Cairo. patients were subjected to full ophthalmological examination, measuring proptosis degree by Hertel’s Exophthalmometer, measuring TRAb serum level. patients were classified according to clinical activity score into 2 groups: Inactive [CAS < 3]: 23 patients received only antithyroid therapy and Active [CAS ≥ 3]: 12 patients received intravenous methylprednisolone at a dose of 0.5gm for 6 weeks, injected weekly. 6 weeks after treatment severity of (GO), proptosis, and TRAb serum level were reassessed. Results: study found the mean CAS was 2.11±1.13, the mean proptosis measured (23.26 ±3.19) and (22.42 ± 3.27) in right and left eye respectively while mean of TRAb was 11.19 ±6.45. After 6 weeks of treatment, CAS was regressed significantly in relation to TRAb level as TRAb measurement decreased by -62.7%, -14.06% in group II and group I respectively while proptosis measurement of right and left eyes in group II significantly decreased, with mean changes of -10.3% and -10.7%, respectively. And, in group I (-4.5% and -3.8%) in right and left eyes respectively, but not significant to TRAb level. Conclusion TRAb level can be used as monitor to activity of Grave’s Ophthalmopathy (GO) and in follow up but not directly related to proptosis degree.
VL - 10
IS - 3
ER -
Abbas, K. N. E. D., Elwan, S., Elsherif, R., Nesim, M., Elsamkary, M. (2025). Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. International Journal of Ophthalmology & Visual Science, 10(3), 42-49. https://doi.org/10.11648/j.ijovs.20251003.11
Abbas, K. N. E. D.; Elwan, S.; Elsherif, R.; Nesim, M.; Elsamkary, M. Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. Int. J. Ophthalmol. Vis. Sci.2025, 10(3), 42-49. doi: 10.11648/j.ijovs.20251003.11
Abbas KNED, Elwan S, Elsherif R, Nesim M, Elsamkary M. Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy. Int J Ophthalmol Vis Sci. 2025;10(3):42-49. doi: 10.11648/j.ijovs.20251003.11
@article{10.11648/j.ijovs.20251003.11,
author = {Karim Nasr El Din Abbas and Sheriff Elwan and Radwa Elsherif and Mina Nesim and Mahmoud Elsamkary},
title = {Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {10},
number = {3},
pages = {42-49},
doi = {10.11648/j.ijovs.20251003.11},
url = {https://doi.org/10.11648/j.ijovs.20251003.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20251003.11},
abstract = {Purpose: evaluating relationship between serum level of TSH Receptor Antibody (TRAb) and severity of Graves’ ophthalmopathy (GO). Methods: prospective interventional follow up study included 35 newly diagnosed untreated patients with GO was carried at Ain Shams University Hospital, Cairo. patients were subjected to full ophthalmological examination, measuring proptosis degree by Hertel’s Exophthalmometer, measuring TRAb serum level. patients were classified according to clinical activity score into 2 groups: Inactive [CAS < 3]: 23 patients received only antithyroid therapy and Active [CAS ≥ 3]: 12 patients received intravenous methylprednisolone at a dose of 0.5gm for 6 weeks, injected weekly. 6 weeks after treatment severity of (GO), proptosis, and TRAb serum level were reassessed. Results: study found the mean CAS was 2.11±1.13, the mean proptosis measured (23.26 ±3.19) and (22.42 ± 3.27) in right and left eye respectively while mean of TRAb was 11.19 ±6.45. After 6 weeks of treatment, CAS was regressed significantly in relation to TRAb level as TRAb measurement decreased by -62.7%, -14.06% in group II and group I respectively while proptosis measurement of right and left eyes in group II significantly decreased, with mean changes of -10.3% and -10.7%, respectively. And, in group I (-4.5% and -3.8%) in right and left eyes respectively, but not significant to TRAb level. Conclusion TRAb level can be used as monitor to activity of Grave’s Ophthalmopathy (GO) and in follow up but not directly related to proptosis degree.},
year = {2025}
}
TY - JOUR
T1 - Correlation Between Serum Level of TSH Receptor Antibody and Severity of Graves’ Orbitopathy
AU - Karim Nasr El Din Abbas
AU - Sheriff Elwan
AU - Radwa Elsherif
AU - Mina Nesim
AU - Mahmoud Elsamkary
Y1 - 2025/07/21
PY - 2025
N1 - https://doi.org/10.11648/j.ijovs.20251003.11
DO - 10.11648/j.ijovs.20251003.11
T2 - International Journal of Ophthalmology & Visual Science
JF - International Journal of Ophthalmology & Visual Science
JO - International Journal of Ophthalmology & Visual Science
SP - 42
EP - 49
PB - Science Publishing Group
SN - 2637-3858
UR - https://doi.org/10.11648/j.ijovs.20251003.11
AB - Purpose: evaluating relationship between serum level of TSH Receptor Antibody (TRAb) and severity of Graves’ ophthalmopathy (GO). Methods: prospective interventional follow up study included 35 newly diagnosed untreated patients with GO was carried at Ain Shams University Hospital, Cairo. patients were subjected to full ophthalmological examination, measuring proptosis degree by Hertel’s Exophthalmometer, measuring TRAb serum level. patients were classified according to clinical activity score into 2 groups: Inactive [CAS < 3]: 23 patients received only antithyroid therapy and Active [CAS ≥ 3]: 12 patients received intravenous methylprednisolone at a dose of 0.5gm for 6 weeks, injected weekly. 6 weeks after treatment severity of (GO), proptosis, and TRAb serum level were reassessed. Results: study found the mean CAS was 2.11±1.13, the mean proptosis measured (23.26 ±3.19) and (22.42 ± 3.27) in right and left eye respectively while mean of TRAb was 11.19 ±6.45. After 6 weeks of treatment, CAS was regressed significantly in relation to TRAb level as TRAb measurement decreased by -62.7%, -14.06% in group II and group I respectively while proptosis measurement of right and left eyes in group II significantly decreased, with mean changes of -10.3% and -10.7%, respectively. And, in group I (-4.5% and -3.8%) in right and left eyes respectively, but not significant to TRAb level. Conclusion TRAb level can be used as monitor to activity of Grave’s Ophthalmopathy (GO) and in follow up but not directly related to proptosis degree.
VL - 10
IS - 3
ER -