Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis
Background: Bladder tumours are a public health problem in Burkina Faso, where they are the second most common urological pathology after prostate cancer. Urinary bilharziasis is a major risk factor in this region. The aim of this study is to analyse the epidemiological and diagnostic characteristics of bladder tumours in the urology department of our Hospital in Burkina Faso. Methods: This is a retrospective study conducted over 3 years (2022-2024) in the urology department. Epidemiological and diagnostic data from 130 patients with bladder tumours were collected and analysed. Data analysis was performed using descriptive statistics, with results presented as frequencies, percentages, and means. Results: The mean age of the patients was 57.55 years. The main risk factors identified were bilharziasis (61.53%) and smoking (26.15%). Haematuria (62.3%) was the main reason for consultation. Histology revealed a predominance of squamous cell carcinomas (79.23%). There was also a significant proportion of urothelial carcinomas (20.77%). The majority of tumours (80%) were diagnosed at an advanced stage. Conclusion: This study highlights the major role played by bilharzia in bladder carcinogenesis in Burkina Faso. Early detection and increased awareness are essential to improve management and reduce the morbidity associated with bladder tumours. The findings underscore the urgent need for strengthened bilharziasis control programs and the implementation of early diagnostic strategies in similar resource-limited, endemic settings.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Bladder tumours are a major public health problem worldwide. They are responsible for 3% of cancer deaths. Their incidence is increasing by around 1% per year, with a greater increase in women than in men
[1]
Roumiguié M, Leon P, Xylinas E, Allory Y, Audenet F, Bajeot AS, et al. French recommendations of the AFU Cancer Committee – 2024–2026 update: non-muscle-invasive bladder tumors (NMIBC). Progress in Urology - FMC. Nov 2024; 34(7): F272-95.
[1]
. Their distribution varies according to region and local risk factors. Globally, urothelial carcinoma is the most common histological type, but in regions where urinary schistosomiasis (bilharziasis) is endemic, such as parts of sub-Saharan Africa, squamous cell carcinoma (SCC) predominates, reflecting the significant influence of environmental and parasitic risk factors on disease pathology.
In sub-Saharan Africa, urinary bilharziasis is a major risk factor, with a predominance of squamous cell carcinomas of the bladder
[2]
Yaméogo CAMKD, Ouédraogo AS, Ouattara A, Kirakoya B, Zongo N, Traoré TM, et al. Urological Cancers in Burkina Faso: Epidemiological and Anatomopathological Aspects of 2204 Cases. OJU. 2020; 10(05): 111-22.
[3]
Niang L, Ndoye M, Labou I, Jalloh M, Diaw J, Thiam I, et al. Epidemiological, clinical and therapeutic aspects of bladder tumors at the Grand Yoff General Hospital in Dakar. African Journal of Urology. Jun 2014; 20(2): 116.
[4]
Diallo T, Bah M, Bah M, Barry A, Kanté D, Cissé D, et al. Epidemiological, clinical and histopathological characteristics of bladder cancers in Conakry. African Urology. Mar 2024; 4(1): 49-49.
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[2-5]
. In recent years, however, there have been notable changes in the proportion of squamous cell carcinomas and urothelial carcinomas. With industrialisation, smoking and improved control of urinary bilharziasis, the relative proportions of squamous cell carcinomas and urothelial carcinomas are shifting in favour of urothelial carcinomas
[6]
Bowa K, Mulele C, Kachimba J, Manda E, Mapulanga V, Mukosai S. A Review of Bladder Cancer in Sub-Saharan Africa: A Different Disease, with a Distinct Presentation, Assessment, and Treatment. Ann Afr Med. 2018; 17(3): 99-105.
[7]
Salem HK, Mahfouz S. Changing Patterns (Age, Incidence, and Pathologic Types) of Schistosoma-associated Bladder Cancer in Egypt in the Past Decade. Urology. Feb 1 2012; 79(2): 379-83.
[6, 7]
. This epidemiological transition underscores the importance of continuous regional surveillance to monitor trends and adapt public health policies accordingly.
In Burkina Faso, bladder tumours are the second most common urological cancer in men after prostate cancer
[2]
Yaméogo CAMKD, Ouédraogo AS, Ouattara A, Kirakoya B, Zongo N, Traoré TM, et al. Urological Cancers in Burkina Faso: Epidemiological and Anatomopathological Aspects of 2204 Cases. OJU. 2020; 10(05): 111-22.
[2]
. Data on trends in the various histological types are limited due to the lack of in-depth epidemiological studies. This study aims to describe the epidemiological and diagnostic aspects of bladder tumours at our Hospital. By providing contemporary local data, this study seeks to contribute to a better understanding of the disease burden and inform local strategies for prevention, diagnosis, and management.
2. Methods
2.1. Study Design and Setting
This is a descriptive study with retrospective data collection conducted over a period of 03 years from 01 January 2022 to 31 December 2024 in the urology department of our Hospital in Burkina Faso, one of the 04 referral hospitals in OUAGADOUGOU.
2.2. Study Population and Inclusion Criteria
The study covered all patients treated for bladder tumours during the period in question. Patients were included if they had a confirmed histological diagnosis of bladder cancer based on transurethral resection of the bladder (TURB) or biopsy specimens. Patients with incomplete medical records or those whose final diagnosis was not bladder cancer were excluded from the analysis.
2.3. Data Collection and Variables
A complete analysis of the patients' medical observations was carried out in order to study the epidemiological and diagnostic aspects of bladder tumours. Data extracted included socio-demographic characteristics (age, sex, occupation), clinical presentation (symptoms, risk factors, physical signs), diagnostic findings (ultrasound, CT scan, cystoscopy), and histopathological results (tumor type, stage, grade). Staging was based on the TNM classification (8th edition) using imaging and histopathological reports.
2.4. Statistical Analysis
Data were analyzed using descriptive statistics. Categorical variables were expressed as frequencies and percentages, and continuous variables (e.g., age) were expressed as means and ranges. Data analysis was performed using Microsoft Excel.
3. Results
3.1. Hospital Frequency of Bladder Tumours
During the study period, 2893 patients were admitted to the urology-andrology department. Of these patients, 178 were admitted for bladder tumours, representing a hospital frequency of 6.15%. After elimination of incomplete and unusable files, 130 were retained. The cases distribution by year is given in the table 1.
Table 1. Distribution of bladder tumour cases by year.
Year
2022
2023
2024
Number of patients
43
35
52
3.2. Socio-Demographic Characteristics of Patients
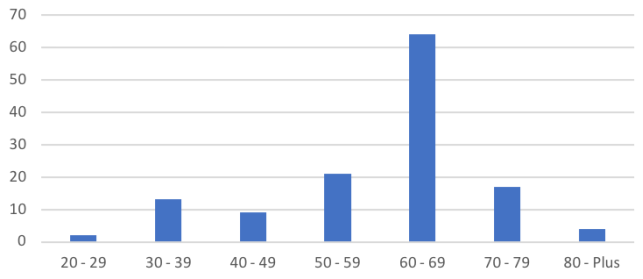
The mean age of the patients was 57.55, with extremes of 43 and 72. The age distribution is shown in Figure 1. The 60 to 69 age group was the most represented (49.23%).
Figure 1. Distribution of patients by age group in years.
In terms of gender, we found that men were in the majority, with 95 men (73.07%) and 35 women (26.92%), corresponding to a sex ratio of 2.71.
In terms of occupation, farmers (rice growers, vegetable growers and cotton growers) were the most represented (56.16%), followed by shopkeepers (13.08%). The other occupations were fishermen (9.24%), livestock farmers (3.84%), housewives (7.69%), civil servants (6.15%) and retired public servants (3.84%).
3.3. Clinical Characteristics of Patients
Risk factors were predominantly bilharziasis (61.53%), followed by smoking (26.15%) and pesticide use (12.32%).
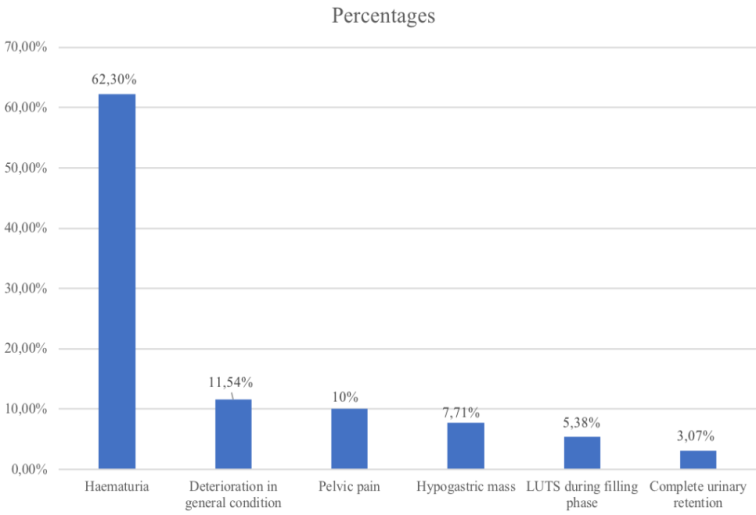
According to consultation reasons, haematuria predominated (62.30%), followed by deterioration in general condition (11.54%) and pelvic pain (10%). Other reasons for consultation were hypogastric masses (7.71%), lower urinary tract symptoms (LUTS) during the filling phase (5.38%) and complete retention of urine (3.07%) (Figure 2).
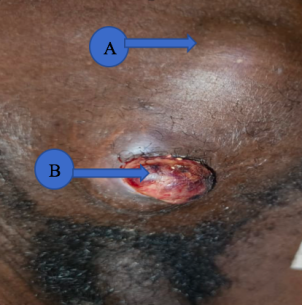
Figure 3. Bladder tumour fistulated to the skin (A: hypogastric mass; B: vesico-cutaneous fistula).
Table 2 shows the distribution according to physical examination data.
Table 2. Distribution according to physical examination data.
Physical signs
Number
Percentage
Hypogastric mass
62
47,69%
Pelvic lymphoedema
9
6,93%
Vesico-cutaneous fistula
3
2,30%
Ascite
03
2,30%
Large kidney
13
10%
Normal
40
30,78%
Total
130
100%
3.4. Paraclinical Characteristics of Patients
All our patients underwent ultrasound of the urinary tract in the first instance to identify the bladder tumour. Seven (07) patients underwent an immediate computed tomography (CT) scan prescribed by general practitioners. We noted 04 cases of focal thickening of the bladder wall, 02 cases of circumferential thickening and 01 case of a prostato-vesical mass whose origin could not be determined on CT.
Ninety-five (95) patients underwent primary urethrocystoscopy to identify the tumour and define its mapping. There were 88 budding tumours and 07 papillary tumours.
The majority of patients (83.07%) underwent their first resection because of the presence of a bladder mass on medical imaging. In 8.47% of patients, the indication was tumour recurrence. Table 3 shows the distribution of patients according to the indication for transurethral resection of the bladder (TURB).
Table 3. Breakdown of patients by indication for transurethral resection of the bladder (TURB).
Indications
Number
Percentage
Bladder mass on imaging
108
83,07%
Second look
03
2,30%
Tumour recurrence
11
8,47%
Incomplete resection
8
6,16%
Total
130
100%
Table 4 shows the cystoscopy data; the tumour was panvesical in 67.70% of cases. The aspect was budding in 64.62% of cases.
Table 4. Distribution according to cystoscopy data.
cystoscopy data
Number (N=130)
Percentage (%)
The number
Unifocal
44
38,85%
Multifocal
86
66,15%
The size
More than 3 cm
104
80%
Less than 3 cm
26
20%
The seat
Trigonal
11
8,47%
Bladder Dome
02
1,53%
Right side
08
6,15%
Left side
09
6,92%
Panvesical
88
67,70%
Rétrotrigonal
12
9,23%
appearance of the tumour
Budding
84
64,62%
Papillary
16
12,30%
Ulcerous-budding
30
23,08%
The histology of the TURB chips in our study showed a predominance of squamous cell carcinomas with 103 cases (79.23%) followed by urothelial carcinomas with 27 cases (20.77%).
For urothelial carcinomas, the tumour infiltrated the muscle in 62.96% of cases compared with 37.04% for tumours not infiltrating the muscle. For squamous cell carcinomas, muscle- invasive bladder cancer (MIBC) were around 95.15% compared with 4.85% of Non-muscle invasive bladder cancer (NMIBC). The distribution of tumors according to the extension assessment is given in Table 5.
In our study, 20% of bladder tumours were localised to the bladder. In the other cases (80%) there was involvement of the peri-vesical fat or neighbouring organs with or without distant metastases.
Table 5. Distribution of tumours according to extension study.
Tumor characteristic
Number (N=130)
Percentage (%)
Tumor localized to the bladder
26
20
Involvement of peri-vesical fat
19
14,61
Tumour invading neighbouring organs
Seminal vesicles
17
13,07
Prostate
24
18,46
Ureters
26
20
Urethra
1
0,76
Abdominal wall
17
13,07
Lymph node metastases
Regional
45
34,61
Non Regional
22
16,92
Distant metastases
16
12,30
4. Discussion
The mean age in our study (57.55 years) is close to that reported by Y. KADOURI et al in Tunisia
[8]
Kadouri Y, Boualaoui I, Lachkar S, Sayegh HE, Benslimane L, Nouini Y. Squamous cell carcinoma of the bladder: retrospective experience in a Moroccan university hospital and literature review. Pan Afr Med J. Oct 8 2020; 37: 143.
[8]
which was 60.4 years. The American Cancer Society states that bladder tumours can occur at a young age, but over 90% occur in people aged over 55
[9]
Cancer Facts & Figures 2006. 1930.
[9]
. This aligns with our findings and is consistent with the global epidemiology of bladder cancer, which primarily affects older adults.
Male predominance has also been found in the literature
[4]
Diallo T, Bah M, Bah M, Barry A, Kanté D, Cissé D, et al. Epidemiological, clinical and histopathological characteristics of bladder cancers in Conakry. African Urology. Mar 2024; 4(1): 49-49.
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[10]
Diao B, Amath T, Fall B, Fall PA, Diémé MJ, Steevy NN, et al. Bladder cancers in Senegal: epidemiological, clinical and histological specificities. Progress in Urology. Jul 2008; 18(7): 445-8.
[4, 5, 10]
, which could be explained by greater exposure to occupational and environmental risk factors, particularly agriculture and the use of pesticides. Farmers were more affected (56.15%) in our series. This could be explained by the fact that the population of Burkina Faso is mainly made up of farmers (rice growers and market gardeners) exposed to urinary bilharziasis, which is the main risk factor for bladder tumours in our country. Our farmers also make extensive use of pesticides. In our study, bilharziasis predominated (61.53%), followed by smoking (26.15%). This can be explained by the fact that urinary bilharziasis is endemic in Burkina Faso. The same is true for Dakar
[3]
Niang L, Ndoye M, Labou I, Jalloh M, Diaw J, Thiam I, et al. Epidemiological, clinical and therapeutic aspects of bladder tumors at the Grand Yoff General Hospital in Dakar. African Journal of Urology. Jun 2014; 20(2): 116.
[3]
and Mali
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[5]
. The presence of schistosoma in the bladder is responsible for cancer. According to EL BOLKAINY et al
[11]
El-Bolkainy MN, Mokhtar NM, Ghoneim MA, Hussein MH. The impact of schistosomiasis on the pathology of bladder carcinoma. Cancer. Dec 15 1981; 48(12): 2643-8.
[11]
, carcinogenesis, a dreadful consequence, appears after a long evolution of the parasitosis. In North African
[12]
Cherif M, Chakroun M, Bouzouita A, Dimassi H, Ayed H, Derouiche A, et al. Epidemiological characteristics of bladder cancer in women in Tunisia. African Journal of Urology. Jun 2016; 22(2): 71-5.
[12]
and Western
[13]
Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of Bladder Cancer. Med Sci (Basel). Mar 13 2020; 8(1): 15.
[13]
countries, smoking remains the main risk factor for bladder tumours.
According to the reason for consultation, haematuria predominated (62.30%), followed by AEG (11.54%) and pelvic pain (10%). Our data corroborate those in the literature
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[14]
Avakoudjo JDG, Yevi DMI, Saidou D, Natchagande G, Hodonou F, Sossa J, et al. Overview of urological tumors at the CNHU-HKM of Cotonou. Journal of the Clinical Biology Society of Benin. 2019; 17-22.
[5, 14]
. These clinical signs of disease generally indicate an advanced tumour. The hypogastric mass was the most frequent physical sign (47.69%). DIALLO et al in Conakry
[4]
Diallo T, Bah M, Bah M, Barry A, Kanté D, Cissé D, et al. Epidemiological, clinical and histopathological characteristics of bladder cancers in Conakry. African Urology. Mar 2024; 4(1): 49-49.
[4]
found a frequency of 18.2%. The presence of a palpable hypogastric mass is a sign of locally advanced tumour, highlighting the delay in consultation in developing countries. This significant delay in presentation, leading to advanced disease stages, is a critical challenge in resource-limited settings and directly impacts treatment options and survival outcomes.
Ninety-five (95) out of 130 patients underwent urethrocystoscopy as part of the diagnostic assessment. Thirty-five (35) patients were diagnosed on the basis of ultrasound or CT scan. According to the recommendations of the Oncology Committee of the French Urology Association, cystoscopy is not mandatory if an imaging examination has already identified the bladder tumour. It is optional in this case
[1]
Roumiguié M, Leon P, Xylinas E, Allory Y, Audenet F, Bajeot AS, et al. French recommendations of the AFU Cancer Committee – 2024–2026 update: non-muscle-invasive bladder tumors (NMIBC). Progress in Urology - FMC. Nov 2024; 34(7): F272-95.
[1]
.
On cystoscopic examination, 67.70% of tumours were panvesical and 80% measured more than 3 cm. This indicates the aggressive nature of the bladder tumours found in our country.
Squamous cell carcinomas were in the majority, accounting for 79.23% of cases compared with 20.77% for urothelial carcinomas. In Senegal, L. NIANG et al
[3]
Niang L, Ndoye M, Labou I, Jalloh M, Diaw J, Thiam I, et al. Epidemiological, clinical and therapeutic aspects of bladder tumors at the Grand Yoff General Hospital in Dakar. African Journal of Urology. Jun 2014; 20(2): 116.
[3]
reported 48.3% squamous cell carcinomas and 37.9% urothelial carcinomas. These results reflect the impact of urinary bilharziasis and confirm the need to strengthen bilharziasis control strategies in order to reduce the incidence of bladder tumours in Africa. Nevertheless, there is a significant proportion of cases of urothelial carcinoma, corroborating data in the literature. For example, in Egypt, a bilharzia-endemic area, the relative proportions of squamous cell carcinomas and urothelial cell carcinomas are shifting in favour of urothelial cell carcinomas
[6]
Bowa K, Mulele C, Kachimba J, Manda E, Mapulanga V, Mukosai S. A Review of Bladder Cancer in Sub-Saharan Africa: A Different Disease, with a Distinct Presentation, Assessment, and Treatment. Ann Afr Med. 2018; 17(3): 99-105.
[7]
Salem HK, Mahfouz S. Changing Patterns (Age, Incidence, and Pathologic Types) of Schistosoma-associated Bladder Cancer in Egypt in the Past Decade. Urology. Feb 1 2012; 79(2): 379-83.
[6, 7]
as a result of industrialisation and improved control of urinary bilharzia. In North African and Western populations, where urinary bilharziasis is rare, urothelial carcinoma predominates
[12]
Cherif M, Chakroun M, Bouzouita A, Dimassi H, Ayed H, Derouiche A, et al. Epidemiological characteristics of bladder cancer in women in Tunisia. African Journal of Urology. Jun 2016; 22(2): 71-5.
[13]
Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of Bladder Cancer. Med Sci (Basel). Mar 13 2020; 8(1): 15.
[12, 13]
. The main risk factors incriminated in these regions were smoking and industrial carcinogens. The high SCC prevalence in our study is a direct reflection of the endemic schistosomiasis, while the presence of UC suggests the influence of other emerging risk factors, akin to the epidemiological transition observed in other endemic regions like Egypt.
For squamous cell carcinomas, MIBC was around 95.15% compared with 4.85% of NMIBC. These data highlight the aggressive and infiltrative nature of squamous cell carcinomas.
In our study, 80% of tumours had spread beyond the bladder muscle and were therefore locally advanced or metastatic. These data, in line with the sub-Saharan African literature
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[10]
Diao B, Amath T, Fall B, Fall PA, Diémé MJ, Steevy NN, et al. Bladder cancers in Senegal: epidemiological, clinical and histological specificities. Progress in Urology. Jul 2008; 18(7): 445-8.
[5, 10]
, highlight the delay in diagnosis in our countries. Early diagnosis would help to reduce the morbidity of these bladder tumours and consequently offer patients better therapeutic alternatives.
This study has limitations inherent to its retrospective design, including potential selection bias and reliance on medical records for data extraction. Furthermore, the single-center nature might limit the generalizability of the findings to the entire country. Nevertheless, it provides valuable insights from a major referral center.
5. Conclusion
This study highlights the epidemiological and diagnostic specificities of bladder tumours at our Hospital, with a high prevalence of bilharziasis as the main risk factor and a predominance of squamous cell carcinoma presenting at advanced stages. The findings strongly advocate for public health strategies focused on two main fronts: firstly, the reinforcement of schistosomiasis control programs to reduce the primary risk factor; and secondly, the implementation of community-based awareness campaigns and accessible diagnostic services to promote earlier detection. Increased awareness among at-risk populations and improved screening strategies are essential to optimise diagnostic results and reduce the morbidity associated with bladder tumours in our context.
Abbreviations
CT
Computed Tomography
MIBC
Muscle Invasive Bladder Cancer
NMIBC
Nonmuscle Invasive Bladder Cancer
TURB
Transurethral Resection of the Bladder
SCC
Squamous Cell Carcinoma
UC
Urothelial Carcinoma
LUTS
Lower Urinary Tract Symptoms
Author Contributions
Clotaire Alexis Marie Kiemdiba Donega Yameogo: Conceptualization, Investigation, Resources, Validation, Writing – original draft, Writing – review & editing
The study was conducted in compliance with the Declaration of Helsinki’s principles on human rights and ethical standards in research and has been approved by CERS (number: 2025-02-50).
Consent for Publication
Consent to publish was obtained from patients.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
References
[1]
Roumiguié M, Leon P, Xylinas E, Allory Y, Audenet F, Bajeot AS, et al. French recommendations of the AFU Cancer Committee – 2024–2026 update: non-muscle-invasive bladder tumors (NMIBC). Progress in Urology - FMC. Nov 2024; 34(7): F272-95.
[2]
Yaméogo CAMKD, Ouédraogo AS, Ouattara A, Kirakoya B, Zongo N, Traoré TM, et al. Urological Cancers in Burkina Faso: Epidemiological and Anatomopathological Aspects of 2204 Cases. OJU. 2020; 10(05): 111-22.
[3]
Niang L, Ndoye M, Labou I, Jalloh M, Diaw J, Thiam I, et al. Epidemiological, clinical and therapeutic aspects of bladder tumors at the Grand Yoff General Hospital in Dakar. African Journal of Urology. Jun 2014; 20(2): 116.
[4]
Diallo T, Bah M, Bah M, Barry A, Kanté D, Cissé D, et al. Epidemiological, clinical and histopathological characteristics of bladder cancers in Conakry. African Urology. Mar 2024; 4(1): 49-49.
[5]
Cisse D, de HSD. Cissé D, Berthé HJG, Diarra A, Coulibaly MT, Diallo MS, Kassogué A, Thiam D, Traore A, Koné M, Guindo O. Bladder Tumors at the Somine Dolo Hospital in Mopti. Health Sci. Dis: Vol 21(10) October 2020 pp 69-74.
[6]
Bowa K, Mulele C, Kachimba J, Manda E, Mapulanga V, Mukosai S. A Review of Bladder Cancer in Sub-Saharan Africa: A Different Disease, with a Distinct Presentation, Assessment, and Treatment. Ann Afr Med. 2018; 17(3): 99-105.
[7]
Salem HK, Mahfouz S. Changing Patterns (Age, Incidence, and Pathologic Types) of Schistosoma-associated Bladder Cancer in Egypt in the Past Decade. Urology. Feb 1 2012; 79(2): 379-83.
[8]
Kadouri Y, Boualaoui I, Lachkar S, Sayegh HE, Benslimane L, Nouini Y. Squamous cell carcinoma of the bladder: retrospective experience in a Moroccan university hospital and literature review. Pan Afr Med J. Oct 8 2020; 37: 143.
[9]
Cancer Facts & Figures 2006. 1930.
[10]
Diao B, Amath T, Fall B, Fall PA, Diémé MJ, Steevy NN, et al. Bladder cancers in Senegal: epidemiological, clinical and histological specificities. Progress in Urology. Jul 2008; 18(7): 445-8.
[11]
El-Bolkainy MN, Mokhtar NM, Ghoneim MA, Hussein MH. The impact of schistosomiasis on the pathology of bladder carcinoma. Cancer. Dec 15 1981; 48(12): 2643-8.
[12]
Cherif M, Chakroun M, Bouzouita A, Dimassi H, Ayed H, Derouiche A, et al. Epidemiological characteristics of bladder cancer in women in Tunisia. African Journal of Urology. Jun 2016; 22(2): 71-5.
[13]
Saginala K, Barsouk A, Aluru JS, Rawla P, Padala SA, Barsouk A. Epidemiology of Bladder Cancer. Med Sci (Basel). Mar 13 2020; 8(1): 15.
[14]
Avakoudjo JDG, Yevi DMI, Saidou D, Natchagande G, Hodonou F, Sossa J, et al. Overview of urological tumors at the CNHU-HKM of Cotonou. Journal of the Clinical Biology Society of Benin. 2019; 17-22.
Yameogo, C. A. M. K. D., Sawadogo, H., Kirakoya, B., Pare, A., Ouattara, A., et al. (2025). Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. International Journal of Clinical Urology, 9(2), 147-153. https://doi.org/10.11648/j.ijcu.20250902.17
Yameogo, C. A. M. K. D.; Sawadogo, H.; Kirakoya, B.; Pare, A.; Ouattara, A., et al. Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. Int. J. Clin. Urol.2025, 9(2), 147-153. doi: 10.11648/j.ijcu.20250902.17
Yameogo CAMKD, Sawadogo H, Kirakoya B, Pare A, Ouattara A, et al. Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. Int J Clin Urol. 2025;9(2):147-153. doi: 10.11648/j.ijcu.20250902.17
@article{10.11648/j.ijcu.20250902.17,
author = {Clotaire Alexis Marie Kiemdiba Donega Yameogo and Hassami Sawadogo and Brahima Kirakoya and Abdoul-Karim Pare and Adama Ouattara and Fasnewinde Aristide Kabore},
title = {Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {147-153},
doi = {10.11648/j.ijcu.20250902.17},
url = {https://doi.org/10.11648/j.ijcu.20250902.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.17},
abstract = {Background: Bladder tumours are a public health problem in Burkina Faso, where they are the second most common urological pathology after prostate cancer. Urinary bilharziasis is a major risk factor in this region. The aim of this study is to analyse the epidemiological and diagnostic characteristics of bladder tumours in the urology department of our Hospital in Burkina Faso. Methods: This is a retrospective study conducted over 3 years (2022-2024) in the urology department. Epidemiological and diagnostic data from 130 patients with bladder tumours were collected and analysed. Data analysis was performed using descriptive statistics, with results presented as frequencies, percentages, and means. Results: The mean age of the patients was 57.55 years. The main risk factors identified were bilharziasis (61.53%) and smoking (26.15%). Haematuria (62.3%) was the main reason for consultation. Histology revealed a predominance of squamous cell carcinomas (79.23%). There was also a significant proportion of urothelial carcinomas (20.77%). The majority of tumours (80%) were diagnosed at an advanced stage. Conclusion: This study highlights the major role played by bilharzia in bladder carcinogenesis in Burkina Faso. Early detection and increased awareness are essential to improve management and reduce the morbidity associated with bladder tumours. The findings underscore the urgent need for strengthened bilharziasis control programs and the implementation of early diagnostic strategies in similar resource-limited, endemic settings.
},
year = {2025}
}
TY - JOUR
T1 - Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Hassami Sawadogo
AU - Brahima Kirakoya
AU - Abdoul-Karim Pare
AU - Adama Ouattara
AU - Fasnewinde Aristide Kabore
Y1 - 2025/10/27
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.17
DO - 10.11648/j.ijcu.20250902.17
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 147
EP - 153
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.17
AB - Background: Bladder tumours are a public health problem in Burkina Faso, where they are the second most common urological pathology after prostate cancer. Urinary bilharziasis is a major risk factor in this region. The aim of this study is to analyse the epidemiological and diagnostic characteristics of bladder tumours in the urology department of our Hospital in Burkina Faso. Methods: This is a retrospective study conducted over 3 years (2022-2024) in the urology department. Epidemiological and diagnostic data from 130 patients with bladder tumours were collected and analysed. Data analysis was performed using descriptive statistics, with results presented as frequencies, percentages, and means. Results: The mean age of the patients was 57.55 years. The main risk factors identified were bilharziasis (61.53%) and smoking (26.15%). Haematuria (62.3%) was the main reason for consultation. Histology revealed a predominance of squamous cell carcinomas (79.23%). There was also a significant proportion of urothelial carcinomas (20.77%). The majority of tumours (80%) were diagnosed at an advanced stage. Conclusion: This study highlights the major role played by bilharzia in bladder carcinogenesis in Burkina Faso. Early detection and increased awareness are essential to improve management and reduce the morbidity associated with bladder tumours. The findings underscore the urgent need for strengthened bilharziasis control programs and the implementation of early diagnostic strategies in similar resource-limited, endemic settings.
VL - 9
IS - 2
ER -
Yameogo, C. A. M. K. D., Sawadogo, H., Kirakoya, B., Pare, A., Ouattara, A., et al. (2025). Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. International Journal of Clinical Urology, 9(2), 147-153. https://doi.org/10.11648/j.ijcu.20250902.17
Yameogo, C. A. M. K. D.; Sawadogo, H.; Kirakoya, B.; Pare, A.; Ouattara, A., et al. Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. Int. J. Clin. Urol.2025, 9(2), 147-153. doi: 10.11648/j.ijcu.20250902.17
Yameogo CAMKD, Sawadogo H, Kirakoya B, Pare A, Ouattara A, et al. Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis. Int J Clin Urol. 2025;9(2):147-153. doi: 10.11648/j.ijcu.20250902.17
@article{10.11648/j.ijcu.20250902.17,
author = {Clotaire Alexis Marie Kiemdiba Donega Yameogo and Hassami Sawadogo and Brahima Kirakoya and Abdoul-Karim Pare and Adama Ouattara and Fasnewinde Aristide Kabore},
title = {Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {2},
pages = {147-153},
doi = {10.11648/j.ijcu.20250902.17},
url = {https://doi.org/10.11648/j.ijcu.20250902.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250902.17},
abstract = {Background: Bladder tumours are a public health problem in Burkina Faso, where they are the second most common urological pathology after prostate cancer. Urinary bilharziasis is a major risk factor in this region. The aim of this study is to analyse the epidemiological and diagnostic characteristics of bladder tumours in the urology department of our Hospital in Burkina Faso. Methods: This is a retrospective study conducted over 3 years (2022-2024) in the urology department. Epidemiological and diagnostic data from 130 patients with bladder tumours were collected and analysed. Data analysis was performed using descriptive statistics, with results presented as frequencies, percentages, and means. Results: The mean age of the patients was 57.55 years. The main risk factors identified were bilharziasis (61.53%) and smoking (26.15%). Haematuria (62.3%) was the main reason for consultation. Histology revealed a predominance of squamous cell carcinomas (79.23%). There was also a significant proportion of urothelial carcinomas (20.77%). The majority of tumours (80%) were diagnosed at an advanced stage. Conclusion: This study highlights the major role played by bilharzia in bladder carcinogenesis in Burkina Faso. Early detection and increased awareness are essential to improve management and reduce the morbidity associated with bladder tumours. The findings underscore the urgent need for strengthened bilharziasis control programs and the implementation of early diagnostic strategies in similar resource-limited, endemic settings.
},
year = {2025}
}
TY - JOUR
T1 - Epidemiological and Diagnostic Aspects of Bladder Tumours in the Urology Department of a Tertiary Care Center in Burkina Faso: A 3-Year Retrospective Analysis
AU - Clotaire Alexis Marie Kiemdiba Donega Yameogo
AU - Hassami Sawadogo
AU - Brahima Kirakoya
AU - Abdoul-Karim Pare
AU - Adama Ouattara
AU - Fasnewinde Aristide Kabore
Y1 - 2025/10/27
PY - 2025
N1 - https://doi.org/10.11648/j.ijcu.20250902.17
DO - 10.11648/j.ijcu.20250902.17
T2 - International Journal of Clinical Urology
JF - International Journal of Clinical Urology
JO - International Journal of Clinical Urology
SP - 147
EP - 153
PB - Science Publishing Group
SN - 2640-1355
UR - https://doi.org/10.11648/j.ijcu.20250902.17
AB - Background: Bladder tumours are a public health problem in Burkina Faso, where they are the second most common urological pathology after prostate cancer. Urinary bilharziasis is a major risk factor in this region. The aim of this study is to analyse the epidemiological and diagnostic characteristics of bladder tumours in the urology department of our Hospital in Burkina Faso. Methods: This is a retrospective study conducted over 3 years (2022-2024) in the urology department. Epidemiological and diagnostic data from 130 patients with bladder tumours were collected and analysed. Data analysis was performed using descriptive statistics, with results presented as frequencies, percentages, and means. Results: The mean age of the patients was 57.55 years. The main risk factors identified were bilharziasis (61.53%) and smoking (26.15%). Haematuria (62.3%) was the main reason for consultation. Histology revealed a predominance of squamous cell carcinomas (79.23%). There was also a significant proportion of urothelial carcinomas (20.77%). The majority of tumours (80%) were diagnosed at an advanced stage. Conclusion: This study highlights the major role played by bilharzia in bladder carcinogenesis in Burkina Faso. Early detection and increased awareness are essential to improve management and reduce the morbidity associated with bladder tumours. The findings underscore the urgent need for strengthened bilharziasis control programs and the implementation of early diagnostic strategies in similar resource-limited, endemic settings.
VL - 9
IS - 2
ER -