Abstract
Background: Dengue, an emerging public health threat, has increased incidence, severity, and geographical spread in Bangladesh. In 2023, the dengue outbreak, 321,179 confirmed cases and 1,705 deaths were reported. This study aimed to project the potential scale and risk distribution of dengue outbreak in 2025 to guide pre-monsoon preparedness. Methods: Using artificial intelligence, we conducted a retrospective epidemiological analysis using national surveillance data from the Directorate General of Health Services (DGHS), Institute of Epidemiology, Disease Control and Research (IEDCR), and WHO reports from 2014 to June 2025. The annual reported dengue case counts, deaths, serotype data, and seasonal patterns were included in the analysis. Projections for 2025 were developed by comparing early-season trends and historical burden across divisions. Results: Between 2014 and 2024, Bangladesh reported an exponential rise in dengue, with the CFR increasing from 0.16% (2019) to 0.57% (2024). In 2025, dengue cases will be expanded to all 64 districts, with new rural hotspots in Barishal, Chattogram, and Khulna divisions. DENV3 and DENV2 will be the dominant circulating serotypes. In 2025, dengue infection is projected to result in 2,82,000–7,91,000 cases and 1,240–4,58 deaths, with Dhaka, Barishal, and Chattogram divisions at the highest risk. Conclusion: Our study concluded an earlier onset, increasing severity, and expanding geographical reach of dengue cases in 2025. Pre-monsoon preparedness—including year-round vector control, clinical readiness, and climate-adaptive planning—is urgently needed to mitigate the anticipated 2025 outbreak.
Keywords
Dengue Epidemiology, Disease Outbreak, Dengue Forecast, Vector Control, Bangladesh
1. Introduction
Dengue fever, a mosquito-borne viral disease caused by four antigenically distinct serotypes of the dengue virus (DENV1, DENV2, DENV3 and DENV4), has emerged as one of the most rapidly spreading arboviral infections globally. Over the last two decades, dengue has become endemic in more than 125 countries, with an estimated 100 million clinical cases and 20,000 deaths reported annually
. The Southeast Asia region, including Bangladesh, bears a disproportionate share of this burden due to favourable ecological, climatic, and urban conditions for the proliferation of Aedes mosquitoes
.
Bangladesh, once considered a low-endemic country for dengue, has witnessed a dramatic epidemiological transformation in the last decade. Since the first recorded dengue outbreak in 2000, the country has experienced intermittent epidemics, primarily localized in Dhaka city. However, the scale and geographical distribution of dengue cases have expanded significantly since 2014. The national health surveillance system reported an exponential rise in dengue cases and deaths, culminating in the unprecedented outbreak of 2023, which recorded 321,179 confirmed cases and 1,705 deaths—more than half of the total dengue burden over the past ten years in the country
.
A significant shift in dengue epidemiology has occurred, with transmission no longer confined to Dhaka. Dengue has now spread to all 64 districts, including rural and peri-urban areas previously considered non-endemic
. Recent data indicate that over 50% of dengue cases in 2023 occurred outside Dhaka, with new hotspots emerging in Chattogram, Barishal, and Khulna divisions. This expansion is attributed to increased human mobility, unplanned urbanisation, and the remarkable adaptive capacity of
Aedes aegypti and
Aedes albopictus mosquitoes to diverse environments
| [5] | Hossain K, Chowdhury S, Shanta IS, Hossain MS, Ghosh PK, Alam MS. Spatio-temporal patterns of dengue in Bangladesh during 2019 to 2023: Implications for targeted control strategies. PLoS Negl Trop Dis. 2024 Sep 20; 18(9): e0012503. https://doi.org/10.1371/journal.pntd.0012503 |
[5]
.
Climatic variables play a pivotal role in dengue transmission. The optimal temperature range for
Aedes mosquito breeding and viral replication (23–29°C) aligns closely with the monsoon and post-monsoon seasons of Bangladesh
. The monsoon period (July to October) consistently witnesses the peak in dengue cases. However, the early surge in 2025 suggests a potential lengthening of the transmission season. Climate change, leading to prolonged humidity and fluctuating rainfall patterns, is likely contributing to this shift
| [7] | Morin CW, Comrie AC, Ernst K. Climate and dengue transmission: evidence and implications. Environ Health Perspect. 2013; 121(11–12): 1264–72. https://doi.org/10.1289/ehp.1306556 |
[7]
.
The persistent co-circulation of multiple serotypes, especially DENV3 and DENV2, has increased the risk of secondary infections, which are strongly associated with severe clinical outcomes such as Dengue Hemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS)
. This immunological dynamic, combined with healthcare system strain and late presentations, may partly explain the rise in case fatality rates—from 0.16% in 2019 to 0.57% in 2024
.
Despite growing severity of dengue, national response strategies have mainly remained reactive, focusing on seasonal vector control and emergency clinical care during peak months. The emerging pattern of early transmission, geographical spread, and rising fatalities underscores the urgent need for a paradigm shift toward proactive, data-driven interventions. This study aimed to assess dengue trends in Bangladesh from 2014 to 2024 and project outbreak risks for 2025 using national surveillance data.
2. Methods
2.1. Study Design
In this study, we used artificial intelligence (AI) to review and analyse data collected from national surveillance sources of Bangladesh, the World Health Organization (WHO), the Centers for Disease Control and Prevention (CDC), and several publications from peer-reviewed journals. It aims to examine dengue trends in Bangladesh from 2014 to 2024 and to project the probable scale and distribution of dengue outbreaks in 2025.
2.2. Study Population
The study population included both urban and rural population across the 64 administrative districts of Bangladesh. No individual patient-level data were used. The analysis focuses on aggregated, publicly reported national and divisional data.
2.3. Data Sources
We used aggregated data from the following sources: a) Annual dengue surveillance reports (2020–2024) from the Directorate General of Health Services (DGHS), b) Outbreak investigation reports and epidemiological briefs from the Institute of Epidemiology, Disease Control and Research (IEDCR), c) Peer-reviewed publications on dengue epidemiology and serotype trends in Bangladesh. c) Weather data (precipitation, temperature, humidity) from the Bangladesh Meteorological Department, d) Entomological assessments and serotype distribution data from icddr,b and relevant field studies. Data included monthly and annual case counts, deaths, CFRs, geographical spread, seasonality patterns, and laboratory serotype surveillance summaries.
2.4. Variables and Definitions
Confirmed dengue case: A case diagnosed using national guidelines, including NS1 antigen, IgM/IgG ELISA, or RT-PCR confirmation, reported through the DGHS surveillance system.
Dengue death: A death occurring in a laboratory-confirmed dengue patient, with dengue listed as the primary cause or a major contributing factor.
Case Fatality Rate (CFR): Defined as the number of dengue-attributed deaths per 100 confirmed dengue cases.
Peak transmission months: Months with the highest recorded number of dengue cases within a given year, typically July to November.
Serotype distribution: Reported laboratory identification of circulating dengue virus serotypes (DENV1–4).
Hotspots and cold spots: Districts with significantly higher or lower dengue incidence per 1,000 population, based on national trends.
2.5. Predictive Modelling Approach
We applied AI-based time series analysis and risk classification algorithms to generate estimates of dengue risk for 2025. The AI tool used Gemini 2.5 pro (Reasoning model) with an extensive prompt to ensure that published data from government websites and only peer-reviewed articles were included. The modelling pipeline included the following steps:
Temporal Pattern Extraction: We used recurrent neural network (RNN)-based architectures, specifically long short-term memory (LSTM) models, to learn seasonal and inter-annual patterns in case data from 2014 to 2024.
Geographic Risk Stratification: District-level risk scores were computed using a composite index combining past case incidence, urban density, vector suitability (inferred from temperature and rainfall thresholds), and serotype replacement events. Clustering methods (e.g., K-means) were used to classify districts within each division as high-risk or relatively lower-risk zones.
Case and Mortality Projections: For each division, we generated point estimates and plausible case ranges using ensemble modelling that incorporated LSTM outputs, historical means, and environmental modifiers. Mortality estimates were derived by applying case fatality ratios (CFRs) observed in 2022–2023 (0.4%–0.6%) to predicted case counts.
Validation and Uncertainty: The models were internally validated using rolling forecasts on withheld 2023–2024 data. Output estimates are reported as ranges to reflect underlying uncertainty and inter-annual variability.
All model development and visualization were conducted in Python 3.9 using open-source libraries (TensorFlow, Scikit-learn, Pandas, NumPy, and Matplotlib).
2.6. Ethical Considerations
This study did not involve human participants or identifiable individual-level data. It relied exclusively on publicly accessible secondary data published by the Government of Bangladesh and international organisations. As such, formal ethical approval was not required. However, the analysis was conducted in line with ethical principles of public health research, ensuring responsible use, accurate citation, and transparent interpretation of data.
3. Results
3.1. Annual Dengue Burden (2014–2024)
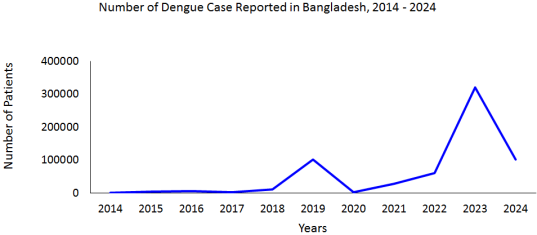
Between 2014 and 2024, Bangladesh experienced a significant escalation in dengue cases and fatalities. The annual number of confirmed dengue cases rose from 375 in 2014 to 321,179 in 2023 (
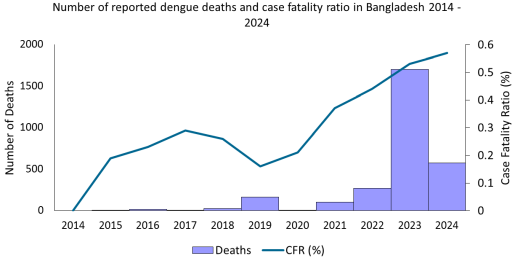
Figure 1). The number of deaths increased from 0 in 2014 to 1,705 in 2023. The Case Fatality Rate (CFR) increased from 0.16% in 2019 to 0.57% in 2024 (
Figure 2).
The five years from 2019 to 2023 accounted for 91.2% of total dengue cases and 96.4% of dengue-related deaths during the ten years. The 2023 outbreak alone contributed 59.9% of all dengue cases and 63.3% of all deaths recorded between 2014 and 2023.
3.2. Projected Dengue Burden and Seasonality in 2025
Dengue transmission in Bangladesh has historically peaked between July and November. The most affected months have consistently been August (26.3%), September (22.5%), and October (20.2%) across 2008–2023. As of June 25, 2025, 8,870 confirmed dengue cases and 36 deaths were reported nationwide.
Figure 1. Distribution of reported dengue cases in Bangladesh, 2014 – 2024.
Figure 2. Distribution of reported dengue deaths and case fatality ratio (%) in Bangladesh, 2014 – 2024.
This represents a threefold increase compared to the same period in 2024 (2,853 cases and 41 deaths by May 25, 2024). The early surge in 2025 indicates an accelerated transmission season, with substantial case burden preceding the typical monsoon peak. The total national burden for 2025 is projected to exceed 2,82,000–7,91,000 cases and 1,240–4,58 deaths (
Table 1).
Table 1. Projected dengue outbreak risk months, duration of outbreaks, cases and deaths by divisions of Bangladesh, 2025.
Divisions | Risk months | Probability (High/ Medium/ Low) | Probable Number of Affected populations (Cases) | Probable number of dengue deaths | Probable Duration of outbreak (months) |
Dhaka | June – November | High | 88,000 – 265,000 | 400 – 1,590 | 5 - 6 |
Chattogram | June – November | High | 66,000 – 199,000 | 300 – 1,190 | 5 - 6 |
Barisal | June – November | High | 18,000 – 55,000 | 80 – 330 | 5 - 6 |
Khulna | June – November | High | 34,000 – 103,000 | 150 – 620 | 5 - 6 |
Rajshahi | July – October | Medium | 30,000 – 71,000 | 120 – 360 | 4 - 5 |
Mymensingh | July – October | Medium | 18,000 – 43,000 | 70 – 220 | 4 - 5 |
Rangpur | July – October | Medium to Low | 17,000 – 44,000 | 70 – 220 | 4 - 5 |
Sylhet | August – October | Low | < 11,000 | < 50 | 3 - 4 |
3.3. Serotype Distribution and Mixed Infections
Analysis of dengue serotyping data from IEDCR and other national laboratories from 2012 to 2023 revealed that DENV3 was 57%, DENV2 was 30%, DENV1 was 11% and DENV4 was rare, not detected in recent years. Mixed infections involving multiple serotypes were reported in Dhaka (2018) and Barguna (2024). DENV2–DENV3 co-infections were noted in rural districts in 2024. The cosmopolitan DENV3-I genotype remains the most prevalent strain circulating nationally.
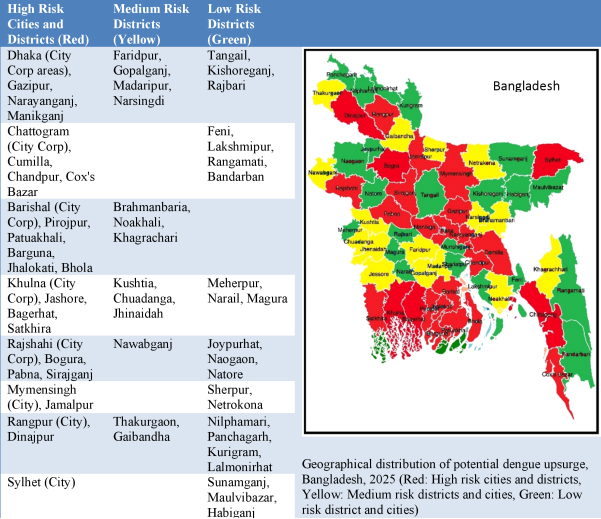
3.4. Geographical Expansion and Shifting Hotspots
In 2023, all 64 districts reported dengue cases. Dhaka Division accounted for 52.7% of cases and 68.2% of deaths. In 2023, Chattogram Division reported 14.2% of national cases, Barishal Division was 11.0%, and Khulna Division was 10.8%. By June 2025, Barishal Division had the highest number of infections outside Dhaka, with Barguna District reporting 2,407 cases and six deaths. Divisions in the southern half of the country (Khulna, Barishal, Chattogram) had a combined dengue incidence of 2.30 per 1,000 population, higher than northern divisions (0.50 per 1,000) and approaching rate of Dhaka (2.90 per 1,000). In contrast, low-incidence ("coldspot") districts included Dinajpur, Gaibandha, Nilphamari, Rangpur, and Sylhet. However, predicted analysis showed that all major cities are at high risk of a dengue outbreak in 2025, along with 26 districts that are at high risk of a dengue outbreak (
Figure 3).
Figure 3. Projected dengue outbreak risk map of Bangladesh, 2025.
4. Discussions
This study highlighted an alarming escalation in dengue incidence and mortality in Bangladesh over the past decade, with the highest burden recorded in 2023 and a strong early surge observed in the first half of 2025. Dengue has also shifted from a Dhaka-centric urban phenomenon to a nationwide public health threat, with new rural and peri-urban hotspots emerging in Barishal, Chattogram, and Khulna divisions. Concurrently, case fatality rates (CFRs) have increased, potentially due to secondary infections with multiple serotypes, health system strain, and delayed treatment in newly affected regions.
The observed rise in dengue burden is not solely attributable to improved surveillance or population growth. Instead, it reflects a fundamental epidemiological transition: dengue has become hyperendemic across Bangladesh. The continued co-circulation of multiple dengue virus serotypes, especially DENV3 and DENV2, significantly raises the risk of severe clinical outcomes due to antibody-dependent enhancement during secondary infections
. In line with this, the CFR increased from 0.16% in 2019 to 0.57% in 2024. A similar pattern has been observed in Brazil and the Philippines, where the emergence of new serotypes or genotype shifts correlated with increased disease severity and deaths
| [10] | Teixeira MG, Siqueira JB Jr, Ferreira GL, Bricks L, Joint G. Epidemiological trends of dengue disease in Brazil (2000–2010): a systematic literature search and analysis. PLoS Negl Trop Dis. 2013; 7(12): e2520. https://doi.org/10.1371/journal.pntd.0002520 |
| [11] | Yoon IK, Srikiatkhachorn A. Immune correlates of protection for dengue: state of the art and research agenda. Vaccine. 2014; 32(26): 3177–83. https://doi.org/10.1016/j.vaccine.2017.07.045 |
[10, 11]
.
The early surge in 2025 case counts strongly suggests that the vector population is already well-established before the typical monsoon onset. This pattern has also been reported in Thailand and Singapore, where climatic variability has extended the dengue season and contributed to early outbreaks
. The consistently warm and humid climate of Bangladesh —particularly during the April to June period—may now support year-round
Aedes mosquito breeding, especially in urban areas where man-made water containers create permanent breeding grounds
| [13] | Brady OJ, Golding N, Pigott DM, et al. Global temperature constraints on Aedes aegypti and Ae. albopictus persistence and competence for dengue virus transmission. Parasit Vectors. 2014; 7: 338. https://doi.org/10.1186/1756-3305-7-338 |
[13]
. This directly impacts the dengue control strategies of the country, which must shift from seasonal fogging and reactive responses to sustained, integrated vector management throughout the year.
The spatial spread of dengue beyond Dhaka to all 64 districts marks a dramatic shift. Our findings show that, in 2023, more than half of all dengue cases occurred outside the capital, with Barguna, Jhalokati, and Cumilla emerging as high-incidence areas. Rural expansion of dengue has also been documented in India, where similar patterns of unplanned urbanisation, internal migration, and inadequate vector control in peri-urban zones have contributed to dengue’s geographical expansion
.
Aedes albopictus, known to bite both day and night and to survive in rural environments, likely plays a larger role in these regions. However, entomological surveillance remains insufficient in Bangladesh, limiting our understanding of vector distribution and behaviour.
Healthcare system capacity is a key determinant of outcomes. During the 2023 outbreak, 67.4% of dengue deaths occurred within one day of hospital admission, indicating either rapid disease progression or late presentation. This trend may disproportionately affect patients in rural and semi-urban areas who face barriers to early diagnosis and referral. Comparable trends were observed in the 2017 outbreak of Sri Lanka, where mortality was strongly associated with delays in care and overwhelmed tertiary hospitals
| [15] | Tissera HA, Jayamanne BDW, Raut R, Janaki SMD, Tozan Y, Samaraweera PC, Liyanage P, Ghouse A, Rodrigo C, de Silva AM, Fernando SD. Severe Dengue Epidemic, Sri Lanka, 2017. Emerg Infect Dis. 2020 Apr; 26(4): 682-691. https://doi.org/10.3201/eid2604.190435 |
[15]
. Addressing these challenges requires decentralisation of clinical care, improved referral pathways, and enhanced training for healthcare workers on early dengue management.
Climate change further complicates the dengue landscape. The average temperature of Bangladesh, during monsoon months (26–31°C), falls within the optimal range for
Aedes mosquito reproduction and virus replication
| [16] | Aguiar M, Anam V, Blyuss KB, Estadilla CDS, Guerrero BV, Knopoff D, Kooi BW, Srivastav AK, Steindorf V, Stollenwerk N. Mathematical models for dengue fever epidemiology: A 10-year systematic review. Phys Life Rev. 2022 Mar; 40: 65-92. https://doi.org/10.1016/j.plrev.2022.02.001 |
[16]
. Increasing rainfall, flooding, and humidity extend this window and may even foster dengue transmission in months previously considered low-risk. A multi-country study by Messina et al. projected a northward and altitudinal expansion of dengue risk areas under climate change scenarios, with South Asia among the most affected regions
. Therefore, climate-resilient urban planning and early warning systems incorporating meteorological data are urgently needed.
The number of dengue cases is increasing day by day [5]. According to current trends, a recent modelling study by Rahman et al. projected that dengue incidence in Bangladesh could reach 500,000 cases per year by 2030
. Our findings align with this trajectory, with projections for 2025 already indicating a possible 400,000–500,000 cases. Similarly, the serotype shift toward DENV3 and mixed infections noted in our study have been observed in Indonesia, where serotype replacement has been linked to hyperendemicity and increased CFRs
| [18] | O’Neill SL, Ryan PA, Turley AP, et al. Scaled deployment of Wolbachia to protect the community from dengue and other Aedes-transmitted arboviruses. Gates Open Res. 2018; 2: 36. https://doi.org/10.12688/gatesopenres.12844.3 |
[18]
. The Government health officials need to be trained in surveillance and advanced statistics for early prediction of cases and application of targeted control measures.
Effective vector control is the mainstay for controlling dengue outbreaks. While studies from Latin America have successfully reduced dengue through Wolbachia-based mosquito interventions, such strategies remain experimental in South Asia
| [18] | O’Neill SL, Ryan PA, Turley AP, et al. Scaled deployment of Wolbachia to protect the community from dengue and other Aedes-transmitted arboviruses. Gates Open Res. 2018; 2: 36. https://doi.org/10.12688/gatesopenres.12844.3 |
[18]
. Current response of Bangladesh depends heavily on fogging and larvicides, which have limited long-term effectiveness without concurrent community engagement and environmental management. The country should invest in conducting entomological research to find out the most effective methods of vector control in the country.
This study had several limitations. First, it relied on secondary surveillance data, which may underreport cases due to asymptomatic infections or limited testing, especially in peripheral regions. Second, the absence of systematic national serotype and genotype surveillance limited the precision of risk projections related to viral evolution. Third, climatic data were not directly modelled in this study but were referenced for contextual interpretation. Lastly, the projected estimates for 2025 are extrapolations based on historical trends and early-season indicators by artificial intelligence; while they are plausible, they should not be interpreted as precise forecasts. We used proper measures for step-by-step analysis and sufficient precautions to prevent the hallucination of data by AI.
5. Conclusion
Based on recent trends and early warning signals, Bangladesh will likely have a widespread dengue outbreak in 2025. The increasing burden, expanding geography, changing climate and rising CFRs highlight the urgent need for a national paradigm shift—from reactive response to sustained, multisectoral, and climate-adaptive dengue preparedness. This study also envisioned using artificial intelligence to predict future outbreaks using published data.
Abbreviations
AI | Artificial Intelligence |
CDC | Centers for Disease Control and Prevention |
CFR | Case Fatality Rate |
DENV | Dengue Virus |
DENV1–4 | Dengue Virus Serotypes 1 to 4 |
DGHS | Directorate General of Health Services |
DHF | Dengue Hemorrhagic Fever |
DSS | Dengue Shock Syndrome |
ELISA | Enzyme-Linked Immunosorbent Assay |
IEDCR | Institute of Epidemiology, Disease Control and Research |
LSTM | Long Short-Term Memory |
NS1 | Nonstructural Protein 1 (antigen) |
RNN | Recurrent Neural Network |
RT-PCR | Reverse Transcriptase–Polymerase Chain Reaction |
WHO | World Health Organization |
Acknowledgments
The authors acknowledge IEDCR, DGHS, icddr,b, weather data and all the published articles that were used in the study. We also acknowledge AI tools used in the study.
Author Contributions
Mallick Masum Billah: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing
Nazmun Nahar Shampa: Data curation, Resources, Supervision, Writing – review & editing
Alden Keith Henderson: Data curation, Methodology, Software, Supervision, Writing – review & editing
Funding
The authors declare that there were no funds received to conduct the study.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
World Health Organization. Dengue and severe dengue. Geneva: WHO; 2024.
https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue
(Accessed on April 10, 2025).
|
| [2] |
Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013; 496(7446): 504–7.
https://doi.org/10.1038/nature12060
|
| [3] |
DGHS. Dengue Dashboard - Health Dashboard – DGHS, Bangladesh. Available at:
https://dashboard.dghs.gov.bd/pages/heoc_dengue_v1.php
(Accessed on March 05, 2025).
|
| [4] |
UNICEF Bangladesh. Dengue outbreak situation report, September 2023. Available at:
https://www.unicef.org/media/145341/file/Bangladesh-Dengue-Outbreak-SitRep-No.3-18-September-2023.pdf
(Accessed on August 23, 2025).
|
| [5] |
Hossain K, Chowdhury S, Shanta IS, Hossain MS, Ghosh PK, Alam MS. Spatio-temporal patterns of dengue in Bangladesh during 2019 to 2023: Implications for targeted control strategies. PLoS Negl Trop Dis. 2024 Sep 20; 18(9): e0012503.
https://doi.org/10.1371/journal.pntd.0012503
|
| [6] |
Messina JP, Brady OJ, Golding N, et al. The current and future global distribution and population at risk of dengue. Nat Microbiol. 2019; 4(9): 1508–15.
https://doi.org/10.1038/s41564-019-0476-8
|
| [7] |
Morin CW, Comrie AC, Ernst K. Climate and dengue transmission: evidence and implications. Environ Health Perspect. 2013; 121(11–12): 1264–72.
https://doi.org/10.1289/ehp.1306556
|
| [8] |
Martina BE, Koraka P, Osterhaus AD. Dengue virus pathogenesis: an integrated view. Clin Microbiol Rev. 2009; 22(4): 564–81.
https://doi.org/10.1128/CMR.00035-09
|
| [9] |
Halstead SB. Dengue. Lancet. 2007; 370(9599): 1644–52.
https://doi.org/10.1016/S0140-6736(07)61687-0
|
| [10] |
Teixeira MG, Siqueira JB Jr, Ferreira GL, Bricks L, Joint G. Epidemiological trends of dengue disease in Brazil (2000–2010): a systematic literature search and analysis. PLoS Negl Trop Dis. 2013; 7(12): e2520.
https://doi.org/10.1371/journal.pntd.0002520
|
| [11] |
Yoon IK, Srikiatkhachorn A. Immune correlates of protection for dengue: state of the art and research agenda. Vaccine. 2014; 32(26): 3177–83.
https://doi.org/10.1016/j.vaccine.2017.07.045
|
| [12] |
Johansson MA, Dominici F, Glass GE. Local and global effects of climate on dengue transmission in Puerto Rico. PLoS Negl Trop Dis. 2009; 3(2): e382.
https://doi.org/10.1371/journal.pntd.0000382
|
| [13] |
Brady OJ, Golding N, Pigott DM, et al. Global temperature constraints on Aedes aegypti and Ae. albopictus persistence and competence for dengue virus transmission. Parasit Vectors. 2014; 7: 338.
https://doi.org/10.1186/1756-3305-7-338
|
| [14] |
Patil RR, Kumar R. Dengue epidemiology in India: a systematic review and meta-analysis. J Med Virol. 2021; 93(3): 1371–85.
https://doi.org/10.1371/journal.pntd.0006618
|
| [15] |
Tissera HA, Jayamanne BDW, Raut R, Janaki SMD, Tozan Y, Samaraweera PC, Liyanage P, Ghouse A, Rodrigo C, de Silva AM, Fernando SD. Severe Dengue Epidemic, Sri Lanka, 2017. Emerg Infect Dis. 2020 Apr; 26(4): 682-691.
https://doi.org/10.3201/eid2604.190435
|
| [16] |
Aguiar M, Anam V, Blyuss KB, Estadilla CDS, Guerrero BV, Knopoff D, Kooi BW, Srivastav AK, Steindorf V, Stollenwerk N. Mathematical models for dengue fever epidemiology: A 10-year systematic review. Phys Life Rev. 2022 Mar; 40: 65-92.
https://doi.org/10.1016/j.plrev.2022.02.001
|
| [17] |
World Meteorological Organization. State of Climate in Asia 2023. Geneva: WMO; 2024. Available at:
https://wmo.int/publication-series/state-of-climate-asia-2023
(accessed August 23, 2025).
|
| [18] |
O’Neill SL, Ryan PA, Turley AP, et al. Scaled deployment of Wolbachia to protect the community from dengue and other Aedes-transmitted arboviruses. Gates Open Res. 2018; 2: 36.
https://doi.org/10.12688/gatesopenres.12844.3
|
Cite This Article
-
APA Style
Billah, M. M., Shampa, N. N., Henderson, A. K. (2025). Escalating Dengue Burden and Emerging Hotspots in Bangladesh: A Decade of Trends and 2025 Forecast. International Journal of Data Science and Analysis, 11(5), 136-142. https://doi.org/10.11648/j.ijdsa.20251105.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Billah, M. M.; Shampa, N. N.; Henderson, A. K. Escalating Dengue Burden and Emerging Hotspots in Bangladesh: A Decade of Trends and 2025 Forecast. Int. J. Data Sci. Anal. 2025, 11(5), 136-142. doi: 10.11648/j.ijdsa.20251105.12
Copy
|
Download
AMA Style
Billah MM, Shampa NN, Henderson AK. Escalating Dengue Burden and Emerging Hotspots in Bangladesh: A Decade of Trends and 2025 Forecast. Int J Data Sci Anal. 2025;11(5):136-142. doi: 10.11648/j.ijdsa.20251105.12
Copy
|
Download
-
@article{10.11648/j.ijdsa.20251105.12,
author = {Mallick Masum Billah and Nazmun Nahar Shampa and Alden Keith Henderson},
title = {Escalating Dengue Burden and Emerging Hotspots in Bangladesh: A Decade of Trends and 2025 Forecast
},
journal = {International Journal of Data Science and Analysis},
volume = {11},
number = {5},
pages = {136-142},
doi = {10.11648/j.ijdsa.20251105.12},
url = {https://doi.org/10.11648/j.ijdsa.20251105.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijdsa.20251105.12},
abstract = {Background: Dengue, an emerging public health threat, has increased incidence, severity, and geographical spread in Bangladesh. In 2023, the dengue outbreak, 321,179 confirmed cases and 1,705 deaths were reported. This study aimed to project the potential scale and risk distribution of dengue outbreak in 2025 to guide pre-monsoon preparedness. Methods: Using artificial intelligence, we conducted a retrospective epidemiological analysis using national surveillance data from the Directorate General of Health Services (DGHS), Institute of Epidemiology, Disease Control and Research (IEDCR), and WHO reports from 2014 to June 2025. The annual reported dengue case counts, deaths, serotype data, and seasonal patterns were included in the analysis. Projections for 2025 were developed by comparing early-season trends and historical burden across divisions. Results: Between 2014 and 2024, Bangladesh reported an exponential rise in dengue, with the CFR increasing from 0.16% (2019) to 0.57% (2024). In 2025, dengue cases will be expanded to all 64 districts, with new rural hotspots in Barishal, Chattogram, and Khulna divisions. DENV3 and DENV2 will be the dominant circulating serotypes. In 2025, dengue infection is projected to result in 2,82,000–7,91,000 cases and 1,240–4,58 deaths, with Dhaka, Barishal, and Chattogram divisions at the highest risk. Conclusion: Our study concluded an earlier onset, increasing severity, and expanding geographical reach of dengue cases in 2025. Pre-monsoon preparedness—including year-round vector control, clinical readiness, and climate-adaptive planning—is urgently needed to mitigate the anticipated 2025 outbreak.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Escalating Dengue Burden and Emerging Hotspots in Bangladesh: A Decade of Trends and 2025 Forecast
AU - Mallick Masum Billah
AU - Nazmun Nahar Shampa
AU - Alden Keith Henderson
Y1 - 2025/09/19
PY - 2025
N1 - https://doi.org/10.11648/j.ijdsa.20251105.12
DO - 10.11648/j.ijdsa.20251105.12
T2 - International Journal of Data Science and Analysis
JF - International Journal of Data Science and Analysis
JO - International Journal of Data Science and Analysis
SP - 136
EP - 142
PB - Science Publishing Group
SN - 2575-1891
UR - https://doi.org/10.11648/j.ijdsa.20251105.12
AB - Background: Dengue, an emerging public health threat, has increased incidence, severity, and geographical spread in Bangladesh. In 2023, the dengue outbreak, 321,179 confirmed cases and 1,705 deaths were reported. This study aimed to project the potential scale and risk distribution of dengue outbreak in 2025 to guide pre-monsoon preparedness. Methods: Using artificial intelligence, we conducted a retrospective epidemiological analysis using national surveillance data from the Directorate General of Health Services (DGHS), Institute of Epidemiology, Disease Control and Research (IEDCR), and WHO reports from 2014 to June 2025. The annual reported dengue case counts, deaths, serotype data, and seasonal patterns were included in the analysis. Projections for 2025 were developed by comparing early-season trends and historical burden across divisions. Results: Between 2014 and 2024, Bangladesh reported an exponential rise in dengue, with the CFR increasing from 0.16% (2019) to 0.57% (2024). In 2025, dengue cases will be expanded to all 64 districts, with new rural hotspots in Barishal, Chattogram, and Khulna divisions. DENV3 and DENV2 will be the dominant circulating serotypes. In 2025, dengue infection is projected to result in 2,82,000–7,91,000 cases and 1,240–4,58 deaths, with Dhaka, Barishal, and Chattogram divisions at the highest risk. Conclusion: Our study concluded an earlier onset, increasing severity, and expanding geographical reach of dengue cases in 2025. Pre-monsoon preparedness—including year-round vector control, clinical readiness, and climate-adaptive planning—is urgently needed to mitigate the anticipated 2025 outbreak.
VL - 11
IS - 5
ER -
Copy
|
Download